

Generation of Epstein-Barr virus-specific cytotoxic T lymphocytes resistant to the immunosuppressive drug tacrolimus (FK506)
- PMID: 19759356
- PMCID: PMC2786289
- DOI: 10.1182/blood-2009-07-230482
Generation of Epstein-Barr virus-specific cytotoxic T lymphocytes resistant to the immunosuppressive drug tacrolimus (FK506)
Abstract
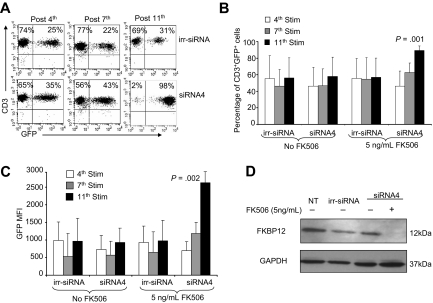
Adoptive transfer of autologous Epstein-Barr virus-specific cytotoxic T lymphocytes (EBV-CTLs) to solid organ transplant (SOT) recipients has been shown safe and effective for the treatment of EBV-associated posttransplantation lymphoproliferative disorders (PTLDs). SOT recipients, however, require the continuous administration of immunosuppressive drugs to prevent graft rejection, and these agents may significantly limit the long-term persistence of transferred EBV-CTLs, precluding their use as prophylaxis. Tacrolimus (FK506) is one of the most widely used immunosuppressive agents in SOT recipients, and its immunosuppressive effects are largely dependent on its interaction with the 12-kDa FK506-binding protein (FKBP12). We have knocked down the expression of FKBP12 in EBV-CTLs using a specific small interfering RNA (siRNA) stably expressed from a retroviral vector and found that FKBP12-silenced EBV-CTLs are FK506 resistant. These cells continue to expand in the presence of the drug without measurable impairment of their antigen specificity or cytotoxic activity. We confirmed their FK506 resistance and anti-PTLD activity in vivo using a xenogenic mouse model, suggesting that the proposed strategy may be of value to enhance EBV-specific immune surveillance in patients at high risk of PTLD after transplantation.
Figures




Comment in
-
Arming CTLs against immunosuppressors.Blood. 2009 Nov 26;114(23):4759-60. doi: 10.1182/blood-2009-09-244905. Blood. 2009. PMID: 19965696 No abstract available.
References
-
- Heslop HE, Ng CY, Li C, et al. Long-term restoration of immunity against Epstein-Barr virus infection by adoptive transfer of gene-modified virus-specific T lymphocytes. Nat Med. 1996;2(5):551–555. - PubMed
-
- Rooney CM, Smith CA, Ng CY, et al. Infusion of cytotoxic T cells for the prevention and treatment of Epstein-Barr virus-induced lymphoma in allogeneic transplant recipients. Blood. 1998;92(5):1549–1555. - PubMed
-
- Comoli P, Labirio M, Basso S, et al. Infusion of autologous Epstein-Barr virus (EBV)-specific cytotoxic T cells for prevention of EBV-related lymphoproliferative disorder in solid organ transplant recipients with evidence of active virus replication. Blood. 2002;99(7):2592–2598. - PubMed
-
- Haque T, Taylor C, Wilkie GM, et al. Complete regression of posttransplant lymphoproliferative disease using partially HLA-matched Epstein Barr virus-specific cytotoxic T cells. Transplantation. 2001;72(8):1399–1402. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
