

Invasive circuitry-based neurotherapeutics: stereotactic ablation and deep brain stimulation for OCD
- PMID: 19759530
- PMCID: PMC3055421
- DOI: 10.1038/npp.2009.128
Invasive circuitry-based neurotherapeutics: stereotactic ablation and deep brain stimulation for OCD
Abstract
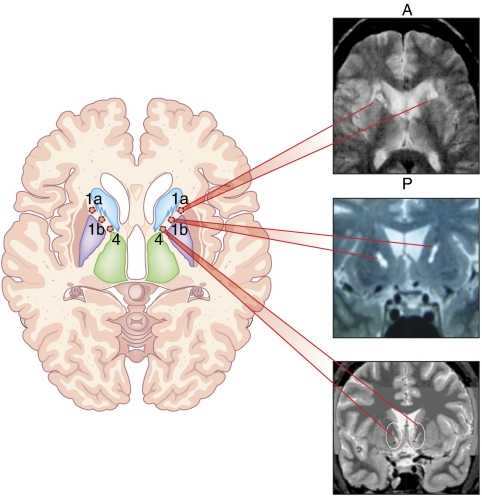
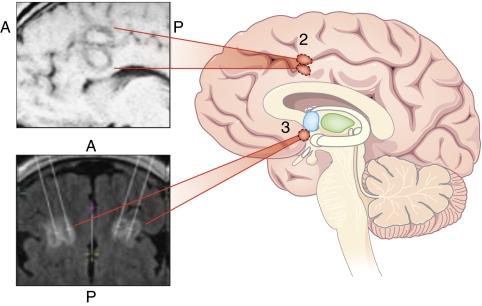
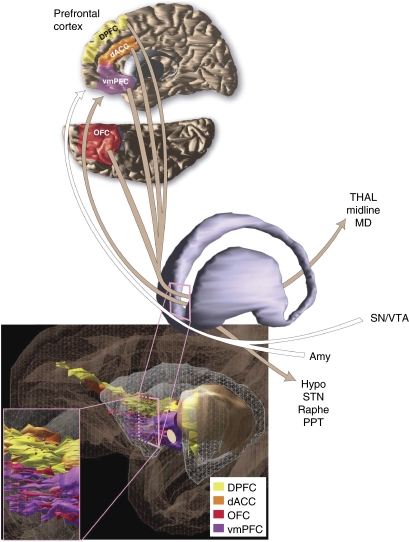
Psychiatric neurosurgery, specifically stereotactic ablation, has continued since the 1940s, mainly at a few centers in Europe and the US. Since the late 1990s, the resurgence of interest in this field has been remarkable; reports of both lesion procedures and the newer technique of deep brain stimulation (DBS) have increased rapidly. In early 2009, the US FDA granted limited humanitarian approval for DBS for otherwise intractable obsessive-compulsive disorder (OCD), the first such approval for a psychiatric illness. Several factors explain the emergence of DBS and continued small-scale use of refined lesion procedures. DBS and stereotactic ablation have been successful and widely used for movement disorders. There remains an unmet clinical need: current drug and behavioral treatments offer limited benefit to some seriously ill people. Understandings of the neurocircuitry underlying psychopathology and the response to treatment, while still works in progress, are much enhanced. Here, we review modern lesion procedures and DBS for OCD in the context of neurocircuitry. A key issue is that clinical benefit can be obtained after surgeries targeting different brain structures. This fits well with anatomical models, in which circuits connecting orbitofrontal cortex (OFC), medial prefrontal cortex (mPFC), basal ganglia, and thalamus are central to OCD pathophysiology and treatment response. As in movement disorders, dedicated interdisciplinary teams, here led by psychiatrists, are required to implement these procedures and maintain care for patients so treated. Available data, although limited, support the promise of stereotactic ablation or DBS in carefully selected patients. Benefit in such cases appears not to be confined to obsessions and compulsions, but includes changes in affective state. Caution is imperative, and key issues in long-term management of psychiatric neurosurgery patients deserve focused attention. DBS and contemporary ablation also present different patterns of potential benefits and burdens. Translational research to elucidate how targeting specific nodes in putative OCD circuitry might lead to therapeutic gains is accelerating in tandem with clinical use.
Figures
References
-
- Abelson JL, Curtis GC, Sagher O, Albucher RC, Harrigan M, Taylor SF, et al. Deep brain stimulation for refractory obsessive-compulsive disorder. Biol Psychiatry. 2005;57:510–516. - PubMed
-
- Albucher RC, Curtis GC, Pitts K. Neurosurgery for obsessive-compulsive disorder: problems with comorbidity. Am J Psychiatry. 1999;156:495–496. - PubMed
-
- Aouizerate B, Cuny E, Martin-Guehl C, Guehl D, Amieva H, Benazzouz A, et al. Deep brain stimulation of the ventral caudate nucleus in the treatment of obsessive-compulsive disorder and major depression. Case report. J Neurosurg. 2004;101:682–686. - PubMed
-
- APA 1994Diagnostic and Statistical Manual of Mental Disorders4th edn.American Psychiatric Association: Washington, DC
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
