

A controversy that has been tough to swallow: is the treatment of achalasia now digested?
- PMID: 19760373
- PMCID: PMC2825313
- DOI: 10.1007/s11605-009-1013-5
A controversy that has been tough to swallow: is the treatment of achalasia now digested?
Abstract
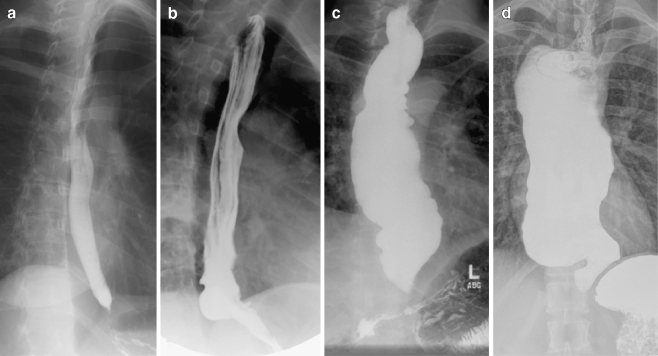
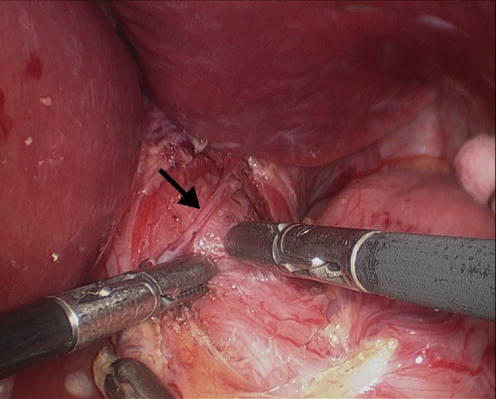
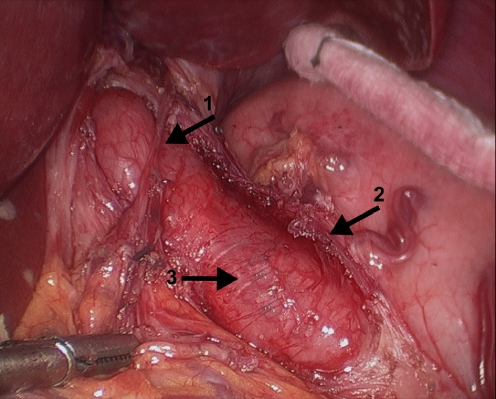
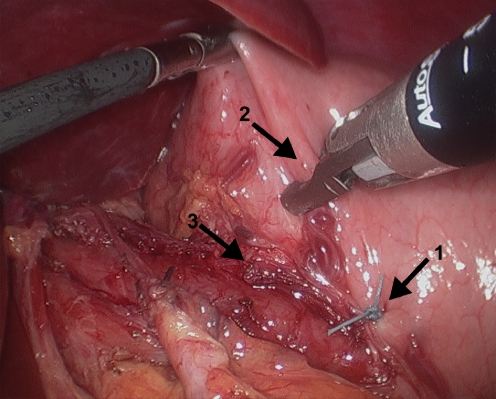
Esophageal achalasia is a rare neurodegenerative disease of the esophagus and the lower esophageal sphincter that presents within a spectrum of disease severity related to progressive pathological changes, most commonly resulting in dysphagia. The pathophysiology of achalasia is still incompletely understood, but recent evidence suggests that degeneration of the postganglionic inhibitory nerves of the myenteric plexus could be due to an infectious or autoimmune mechanism, and nitric oxide is the neurotransmitter affected. Current treatment of achalasia is directed at palliation of symptoms. Therapies include pharmacological therapy, endoscopic injection of botulinum toxin, endoscopic dilation, and surgery. Until the late 1980s, endoscopic dilation was the first line of therapy. The advent of safe and effective minimally invasive surgical techniques in the early 1990s paved the way for the introduction of laparoscopic myotomy. This review will discuss the most up-to-date information regarding the pathophysiology, diagnosis, and treatment of achalasia, including a historical perspective. The laparoscopic Heller myotomy with partial fundoplication performed at an experienced center is currently the first line of therapy because it offers a low complication rate, the most durable symptom relief, and the lowest incidence of postoperative gastroesophageal reflux.
Figures


References
-
- Ruffato A, Mattioli S, Lugaresi ML, Lugaresi ML, D'Ovidio F, Antonacci F, Di Simone MP. Long-term results after Heller–Dor operation for oesophageal achalasia. Eur J Cardiothorac Surg. 2006;29:914–919. - PubMed
-
- Podas T, Eaden J, Mayberry M, Mayberry J. Achalasia: a critical review of epidemiological studies. Am J Gastroenterol. 1998;93:2345–2347. - PubMed
-
- Birgisson S, Richter JE. Achalasia: what's new in diagnosis and treatment? Dig Dis. 1997;15(Suppl 1):1–27. - PubMed
-
- Bennett JR, Hendrix TR. Treatment of achalasia with pneumatic dilatation. Mod Treat. 1970;7:1217–1228. - PubMed
-
- Bonatti H, Hinder RA, Klocker J, Neuhaser B, Klaus A, Achem SR, de Vault K. Long-term results of laparoscopic Heller myotomy with partial fundoplication for the treatment of achalasia. Am J Surg. 2005;190:874–878. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
