

Strategies for the targeted delivery of therapeutics for osteosarcoma
- PMID: 19761419
- PMCID: PMC4163784
- DOI: 10.1517/17425240903280422
Strategies for the targeted delivery of therapeutics for osteosarcoma
Abstract
Background: Conventional therapy for osteosarcoma has reached a plateau of 60 - 70%, a 5-year survival rate that has changed little in two decades, highlighting the need for new approaches.
Objective: To review the alternative means of delivering effective therapy for osteosarcoma that reach beyond the central venous catheter.
Methods: Drawing on the author's own experiences providing care to high-risk osteosarcoma patients and reviewing the last two decades of literature describing sarcoma therapy, available information is summarized about potential osteosarcoma treatments that deliver therapy by a less conventional route.
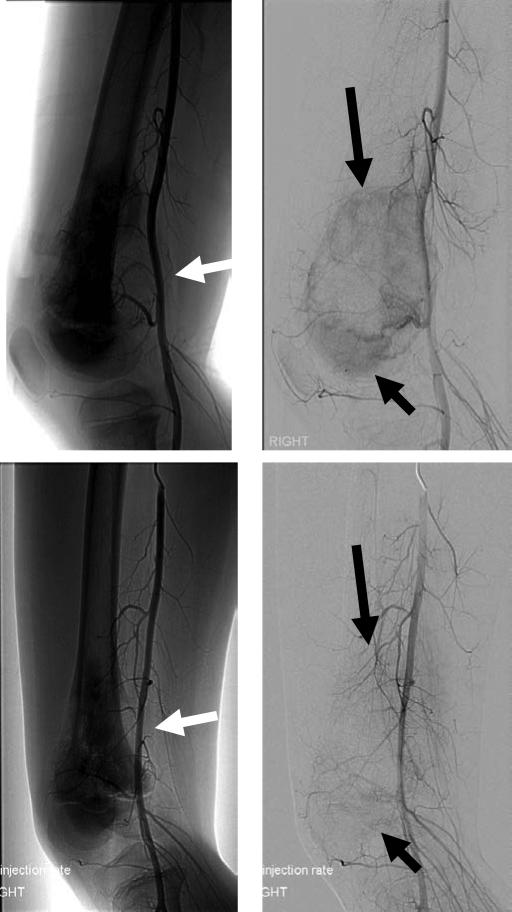
Results/conclusions: Intra-arterial chemotherapy has a limited impact on survival, but may help to achieve a better limb salvage. Intrapleural chemotherapy is important for managing malignant effusions. The development of inhalation therapies, treatments that target new bone formation such as bisphosphonates, chemically targeted radiation and antibody-based therapies all have potential to improve osteosarcoma therapy.
Figures

References
-
- Herzog CE. Overview of sarcomas in the adolescent and young adult population. J Pediatr Hematol Oncol. 2005 Apr 1;27(4):215–8. 2005. - PubMed
-
- Meyer WH, Malawer MM. Osteosarcoma. Clinical features and evolving surgical and chemotherapeutic strategies. Pediatric Clinics of North America. 1991;38(2):317–48. - PubMed
-
- Longhi A, Errani C, De Paolis M, Mercuri M, Bacci G. Primary bone osteosarcoma in the pediatric age: State of the art. Cancer Treat Rev. 2006 Oct 1;32(6):423–36. 2006. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical