

Review
doi: 10.3174/ajnr.A1704.
Epub 2009 Sep 17.
A compartment-based approach for the imaging evaluation of tinnitus
Affiliations
- PMID: 19762464
- PMCID: PMC7964158
- DOI: 10.3174/ajnr.A1704
Item in Clipboard
Review
A compartment-based approach for the imaging evaluation of tinnitus
AJNR Am J Neuroradiol.
2010 Feb.
Abstract
Tinnitus affects 10% of the US general population and is a common indication for imaging studies. We describe a sequential compartment-based diagnostic approach, which simplifies the interpretation of imaging studies in patients with tinnitus. The choice of the initial imaging technique depends on the type of tinnitus, associated symptoms, and examination findings. Familiarity with the pathophysiologic mechanisms of tinnitus and the imaging findings is a prerequisite for a tailored diagnostic approach by the radiologist.
Figures
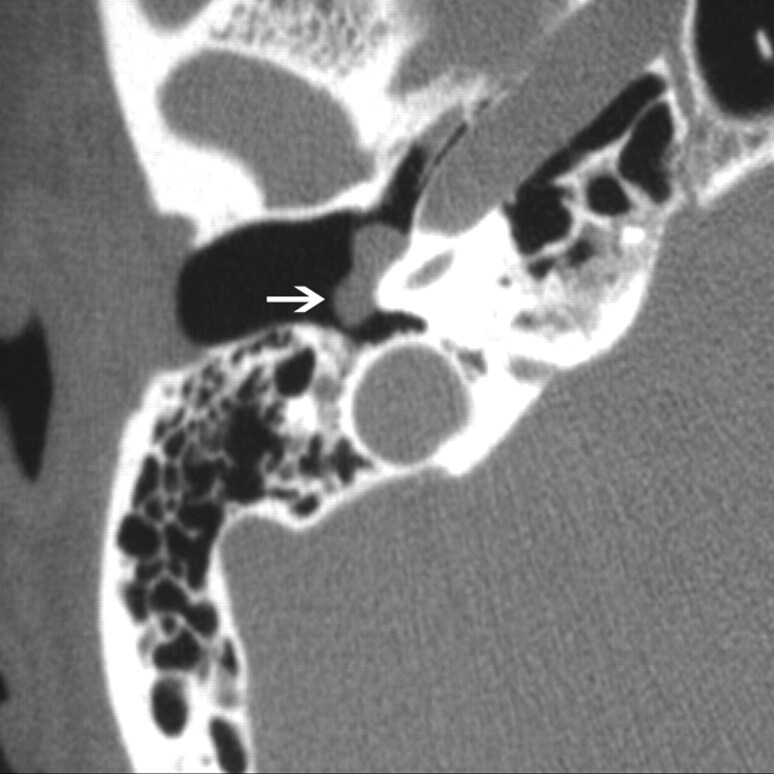
Glomus tympanicum (arrow) in a 30-year-old woman with right-sided pulsatile tinnitus. Axial CT image demonstrates lobulated soft-tissue attenuation in the middle ear overlying the cochlear promontory.
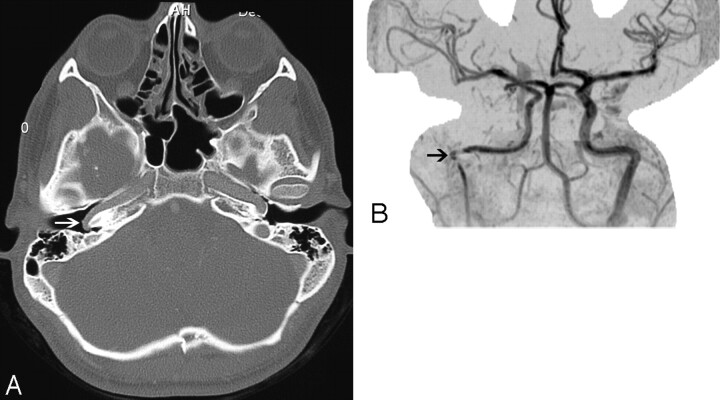
Aberrant course of the ICA in a 25-year-old man presenting with pulsatile tinnitus. A, Enhanced axial CT image demonstrates an abnormal lateral course of the right ICA through the middle ear (white arrow). Also note dehiscence of the overlying bony plate. B, Anteroposterior projection image from the MR angiogram of the same patient demonstrates decreased caliber and lateral deviation of the aberrant ICA on the “right reversed-7 sign” (black arrow).
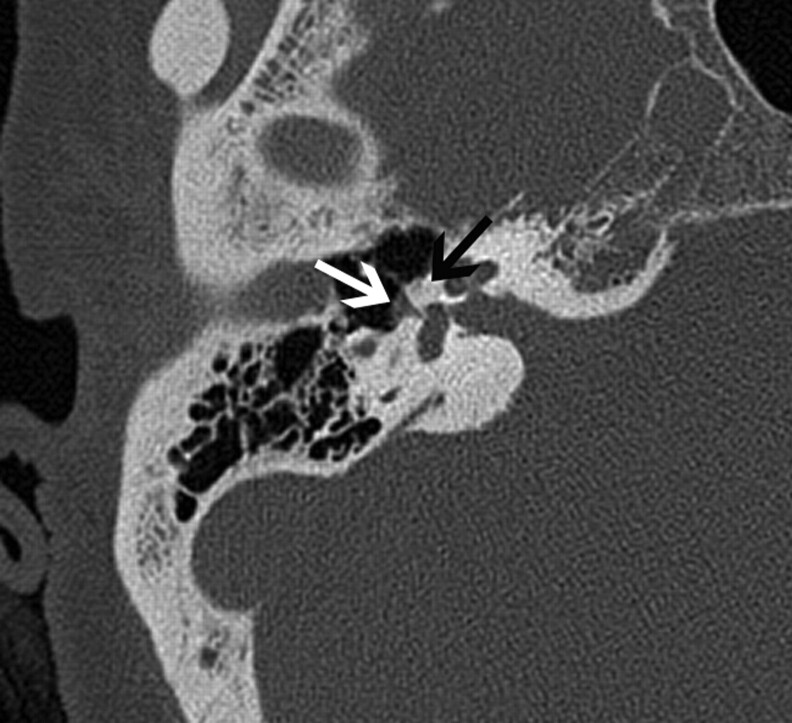
Fenestral otospongiosis in a 35-year-old woman with hearing loss and tinnitus. Axial CT image demonstrates soft-tissue attenuation in the oval window (white arrow) and abnormal lucency at the fissula antefenestram (black arrow).
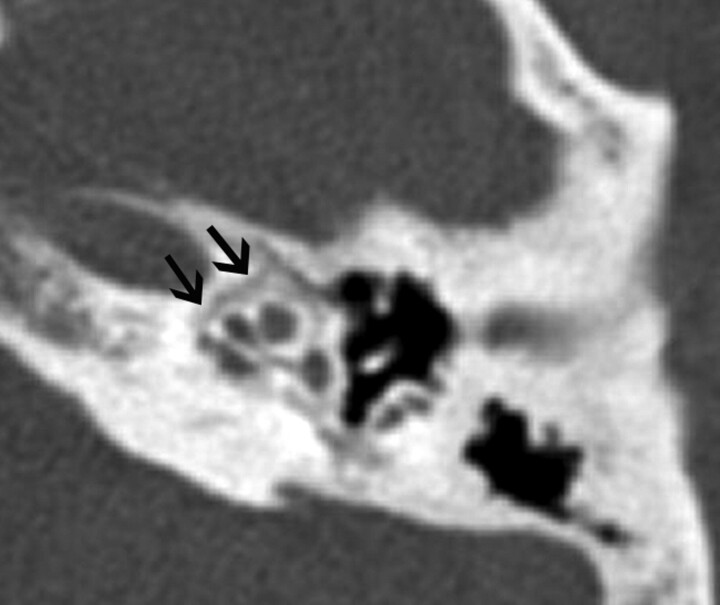
A 50-year-old man with cochlear otospongiosis. Axial CT scan demonstrates abnormal lucency surrounding the left cochlea (black arrows).
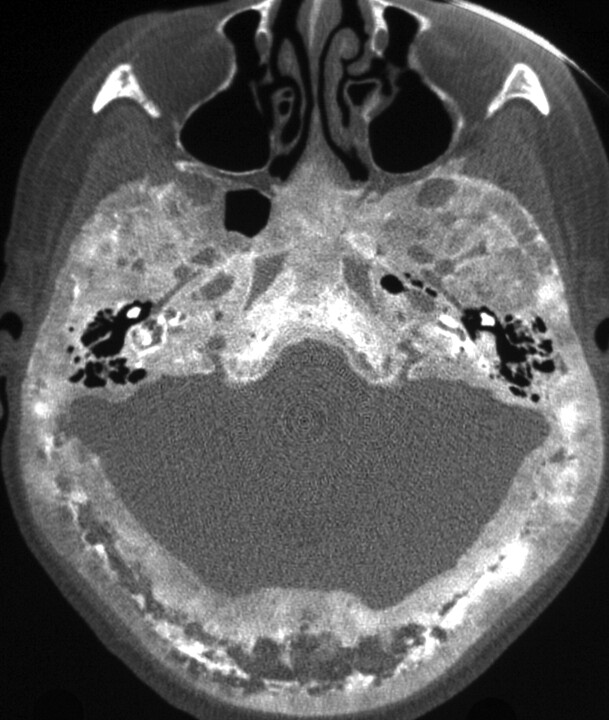
Paget disease of the skull base in a 70-year-old man. Axial CT scan demonstrates diffuse expansion and sclerosis of the bones of the skull base, characteristic of Paget disease. Note the sparing of the maxillofacial bones, which, along with the age of the patient, is a helpful feature in differentiating it from fibrous dysplasia.
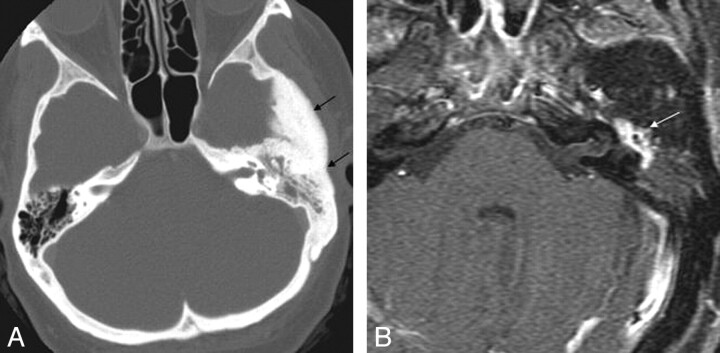
Intraosseous temporal bone meningioma in a 45-year-old woman who presented with left-sided hearing loss and tinnitus. A, Axial CT image demonstrates diffuse sclerosis of the temporal bone and soft-tissue attenuation (black arrows) in the left mastoid and middle ear cavity. B, Axial enhanced MR image in the same patient demonstrates enhancement within the left middle ear (white arrow).
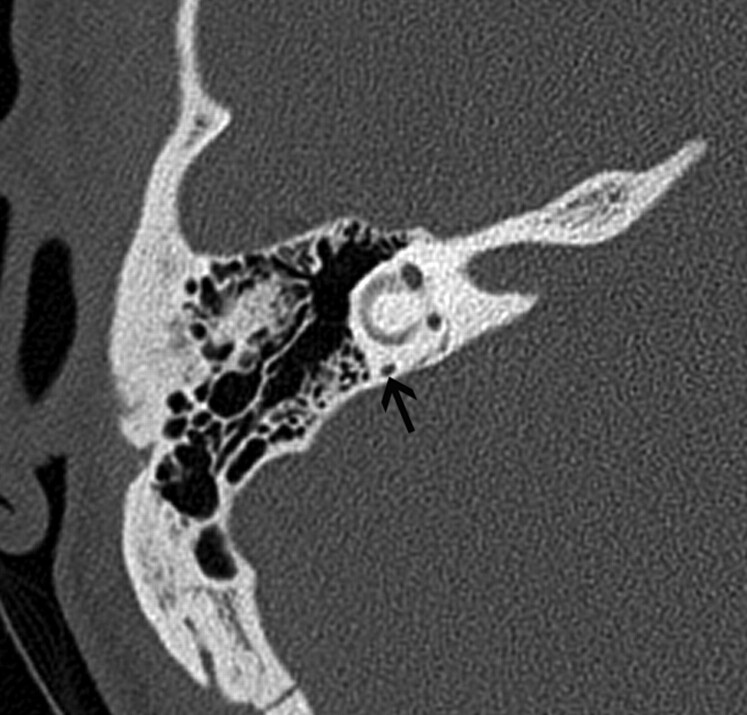
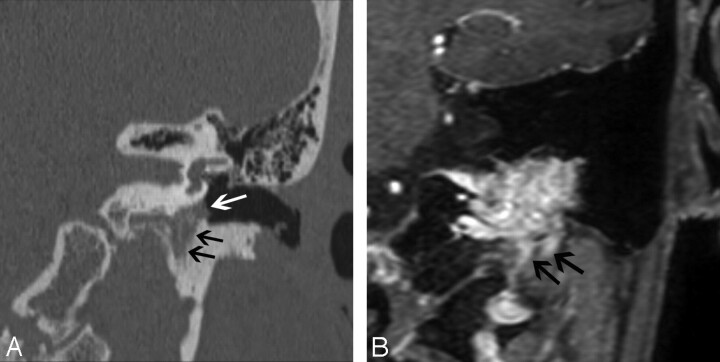
A 50-year-old man with MD. Axial thin-section CT image shows decreased distance between the vertical limb of the posterior semicircular canal and the posterior edge of the temporal bone (black arrow).
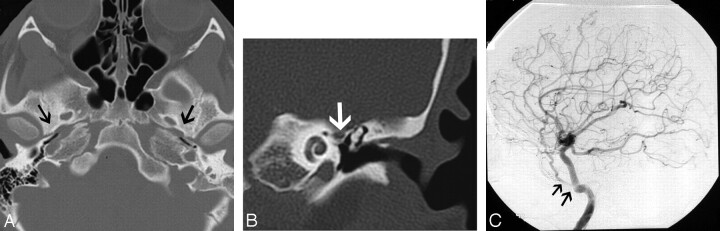
A 30-year-old man with PSA. A, Axial CT image demonstrates absence of the foramen spinosum bilaterally (black arrows). B, Coronal CT image in the same patient shows enlargement of the tympanic part of the facial nerve canal, another indirect imaging sign of PSA. C, Lateral DSA image of the internal carotid injection shows the PSA arising from the ICA (arrows).
Glomus jugulotympanicum in 45-year-old woman who presented with left-sided pulsatile tinnitus. A, Coronal CT image demonstrates soft-tissue attenuation projecting in the hypotympanum (white arrow). There is permeative osseous destruction in the left jugular foramen (black arrows), providing a clue as to the origin of the mass in the left jugular foramen. B, Enhanced coronal MR image better demonstrates the true extent of the mass within the left jugular foramen (black arrows).
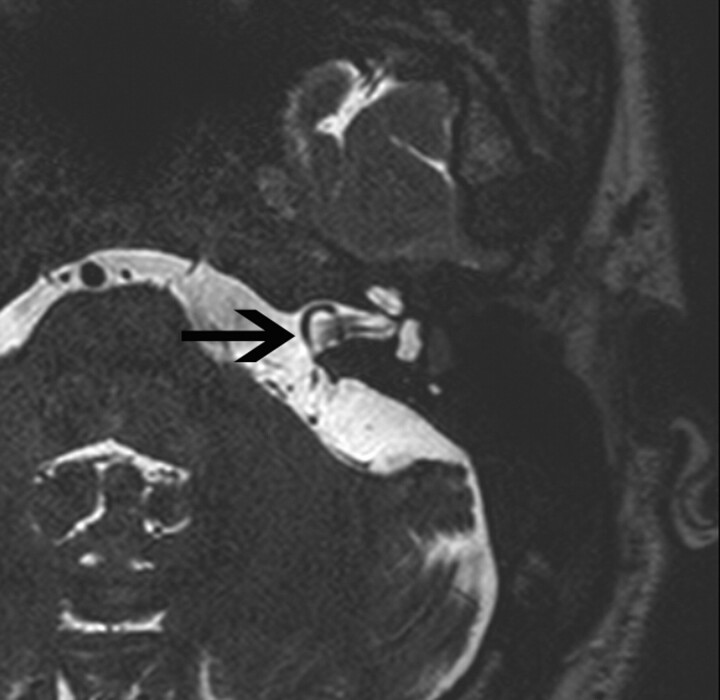
Anterior inferior cerebellar artery loop in a 35-year-old man. Axial T2-weighted MR image shows a vascular loop entering the IAC (black arrow).
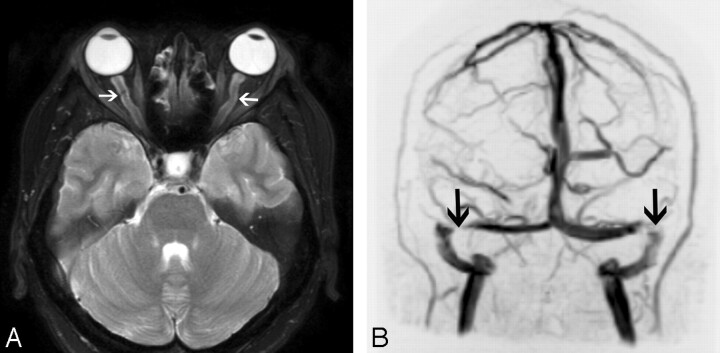
Intracranial hypertension in a 30-year-old woman presenting with headaches and tinnitus. A, Axial T2-weighted image demonstrates dilation of bilateral optic nerve sheaths (arrows) and flattening of the posterior globes. B, Coronal maximum-intensity-projection image from an MR venogram also demonstrates stenoses of bilateral transverse sinuses (arrows).
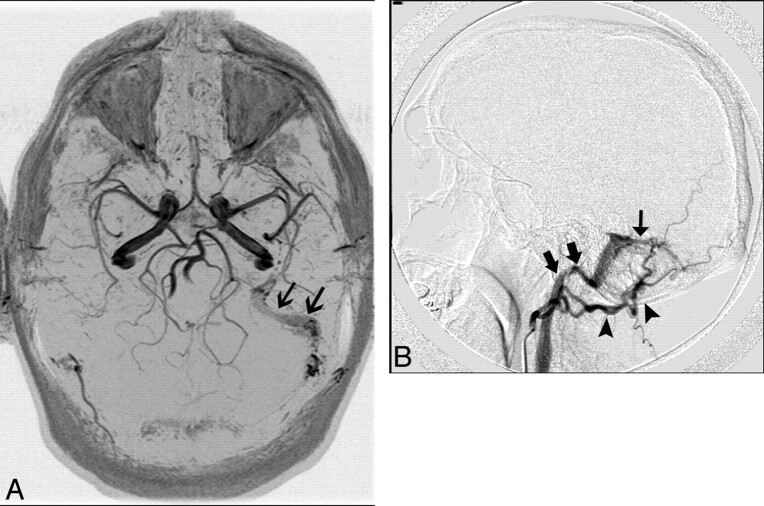
A 40-year-old man who presented with left-sided pulsatile tinnitus. A, MR angiogram demonstrates asymmetric increased flow-related enhancement in the left sigmoid sinus (black arrows) and multiple small arterial flow voids within it. B, Lateral projection of DSA shows injection of the left occipital artery (arrowheads) opacifying the AVF (thin black arrow) and rapid opacification of the left sigmoid sinus and internal jugular vein (thick black arrows).
References
-
- Meyerhoff WL, Cooper JC. Tinnitus. In: Paparella MM. ed. Otolaryngology. 3rd ed. Philadelphia: Saunders; 1991:1169–75
-
- Schleuning AJ, 2nd. Management of the patient with tinnitus. Med Clin North Am 1991;75:1225–37 - PubMed
-
- Lockwood AH, Salvi RJ, Burkard RF. Tinnitus. N Engl J Med 2002;347:904–10 - PubMed
-
- Bauer CA. Mechanisms of tinnitus generation. Curr Opin Otolaryngol Head Neck Surg 2004;12:413–17 - PubMed
-
- Sismanis A. Tinnitus. Curr Neurol Neurosci Rep 2001;1:492–99 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical