

The natural progression of shoulder osteonecrosis related to corticosteroid treatment
- PMID: 19763721
- PMCID: PMC2882009
- DOI: 10.1007/s11999-009-1094-1
The natural progression of shoulder osteonecrosis related to corticosteroid treatment
Abstract
Background: Little is known about the rate and factors of progression of shoulder osteonecrosis (ON) related to corticosteroids.
Purpose: We retrospectively evaluated 125 patients (215 shoulders) with humeral head ON diagnosed by MRI to determine the delay between corticosteroid treatment and the different stages and factors influencing the progression of the disease.
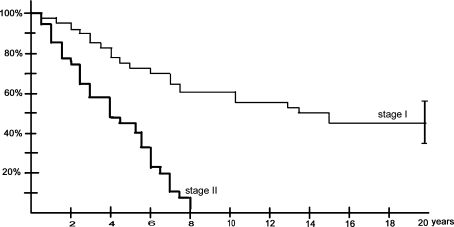
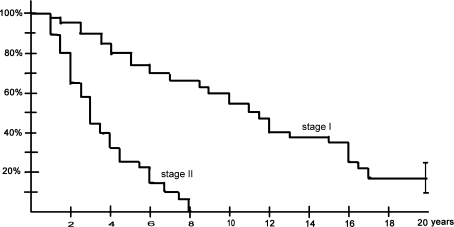
Methods: Seventy-four of the shoulders had asymptomatic Stage I ON, 58 had asymptomatic Stage II ON, 46 had symptomatic Stage I ON, and 37 had symptomatic Stage II ON. The minimum followup was 10 years (average, 14 years; range, 10-20 years). The delay between the beginning of the corticosteroid treatment and the diagnosis of ON of the humeral head averaged 15 months (range, 6-24 months).
Results: We observed partial or total regression on MRI only in patients with asymptomatic Stage I ON. At last followup, pain had developed in 98 (74%) and collapse had occurred in 71 (54%) of the 132 previously asymptomatic shoulders. Of the 83 symptomatic shoulders, 68 (82%) had collapsed at the final followup. The time between diagnosis and collapse averaged 10 years for patients with symptomatic Stage I ON and 3 years for patients with symptomatic Stage II ON.
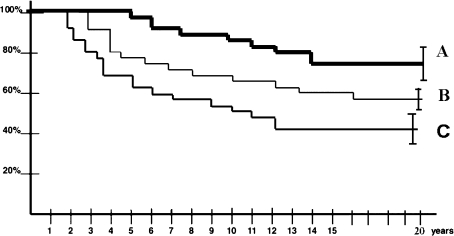
Conclusions: Stage at initial visit, occurrence of pain, and continuation of peak doses of corticosteroids predicted progression of disease in asymptomatic shoulders, whereas in the symptomatic shoulders, extent and location of the lesion were the main risk factors for progression.
Level of evidence: Level II, prognostic study. See Guidelines for Authors for a complete description of levels.
Figures

References
-
- Cheng EY, Thongtrangan I, Laorr A, Saleh KJ. Spontaneous resolution of osteonecrosis of the femoral head. J Bone Joint Surg Am. 2004;86:2594–2599. - PubMed
-
- Cruess RL. Steroid-induced avascular necrosis of the head of the humerus: natural history and management. J Bone Joint Surg Br. 1976;58:313–317. - PubMed
-
- Cruess RL. Experience with steroid-induced avascular necrosis of the shoulder and etiologic considerations regarding osteonecrosis of the hip. Clin Orthop Relat Res. 1978;130:86–93. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
