

Perinatal acquisition of drug-resistant HIV-1 infection: mechanisms and long-term outcome
- PMID: 19765313
- PMCID: PMC2756278
- DOI: 10.1186/1742-4690-6-85
Perinatal acquisition of drug-resistant HIV-1 infection: mechanisms and long-term outcome
Abstract
Background: Primary-HIV-1-infection in newborns that occurs under antiretroviral prophylaxis that is a high risk of drug-resistance acquisition. We examine the frequency and the mechanisms of resistance acquisition at the time of infection in newborns.
Patients and methods: We studied HIV-1-infected infants born between 01 January 1997 and 31 December 2004 and enrolled in the ANRS-EPF cohort. HIV-1-RNA and HIV-1-DNA samples obtained perinatally from the newborn and mother were subjected to population-based and clonal analyses of drug resistance. If positive, serial samples were obtained from the child for resistance testing.
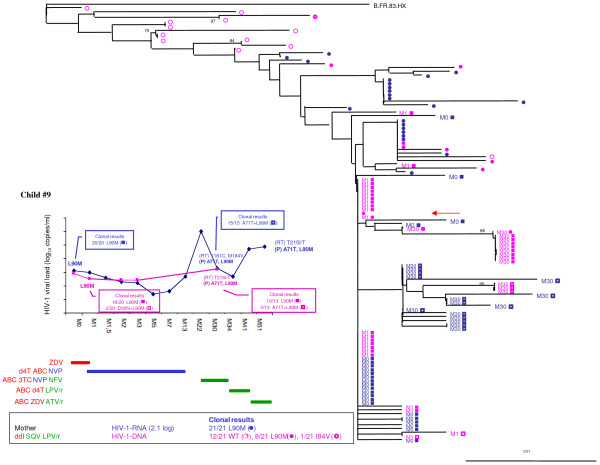
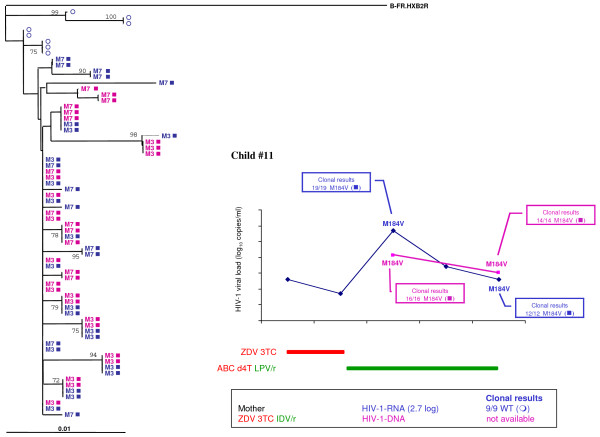
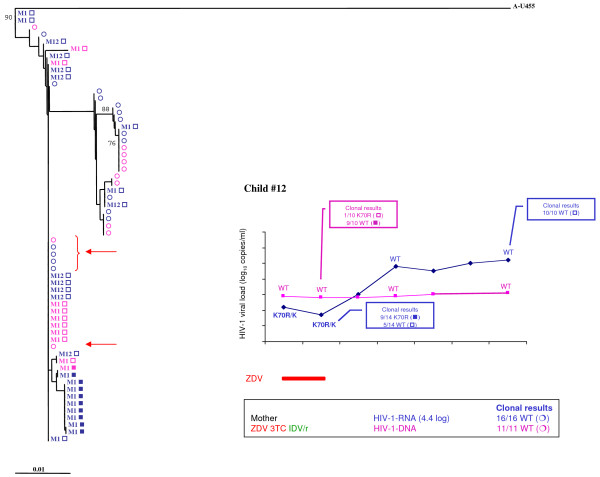
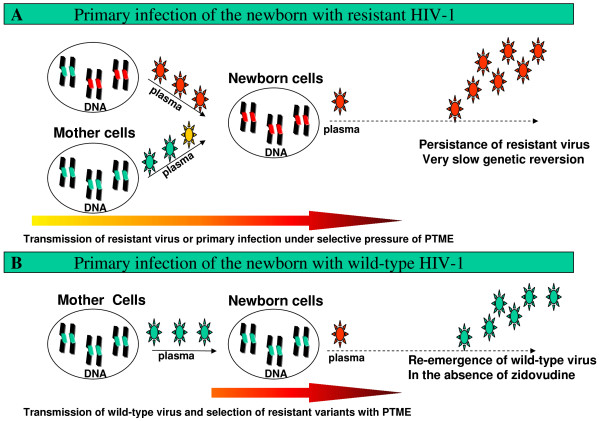
Results: Ninety-two HIV-1-infected infants were born during the study period. Samples were obtained from 32 mother-child pairs and from another 28 newborns. Drug resistance was detected in 12 newborns (20%): drug resistance to nucleoside reverse transcriptase inhibitors was seen in 10 cases, non-nucleoside reverse transcriptase inhibitors in two cases, and protease inhibitors in one case. For 9 children, the detection of the same resistance mutations in mothers' samples (6 among 10 available) and in newborn lymphocytes (6/8) suggests that the newborn was initially infected by a drug-resistant strain. Resistance variants were either transmitted from mother-to-child or selected during subsequent temporal exposure under suboptimal perinatal prophylaxis. Follow-up studies of the infants showed that the resistance pattern remained stable over time, regardless of antiretroviral therapy, suggesting the early cellular archiving of resistant viruses. The absence of resistance in the mother of the other three children (3/10) and neonatal lymphocytes (2/8) suggests that the newborns were infected by a wild-type strain without long-term persistence of resistance when suboptimal prophylaxis was stopped.
Conclusion: This study confirms the importance of early resistance genotyping of HIV-1-infected newborns. In most cases (75%), drug resistance was archived in the cellular reservoir and persisted during infancy, with or without antiretroviral treatment. This finding stresses the need for effective antiretroviral treatment of pregnant women.
Figures
References
-
- Rouzioux C, Costagliola D, Burgard M, Blanche S, Mayaux MJ, Griscelli C, Valleron AJ. Estimated timing of mother-to-child human immunodeficiency virus type 1 (HIV-1) transmission by use of a Markov model. The HIV Infection in Newborns French Collaborative Study Group. Am J Epidemiol. 1995;142:1330–1337. - PubMed
-
- Connor EM, Sperling RS, Gelber R, Kiselev P, Scott G, O'Sullivan MJ, VanDyke R, Bey M, Shearer W, Jacobson RL, et al. Reduction of maternal-infant transmission of human immunodeficiency virus type 1 with zidovudine treatment. Pediatric AIDS Clinical Trials Group Protocol 076 Study Group. N Engl J Med. 1994;331:1173–1180. doi: 10.1056/NEJM199411033311801. - DOI - PubMed
-
- Cooper ER, Charurat M, Mofenson L, Hanson IC, Pitt J, Diaz C, Hayani K, Handelsman E, Smeriglio V, Hoff R, Blattner W. Combination antiretroviral strategies for the treatment of pregnant HIV-1-infected women and prevention of perinatal HIV-1 transmission. J Acquir Immune Defic Syndr. 2002;29:484–494. - PubMed
-
- Yeni P. Prise en charge meìdicale des personnes infecteìes par le VIH Flammarion edn. Paris: Médecine-Sciences; 2008.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
