

Dose-dense temozolomide regimen for the treatment of brain metastases from melanoma, breast cancer, or lung cancer not amenable to surgery or radiosurgery: a multicenter phase II study
- PMID: 19767314
- PMCID: PMC2826096
- DOI: 10.1093/annonc/mdp343
Dose-dense temozolomide regimen for the treatment of brain metastases from melanoma, breast cancer, or lung cancer not amenable to surgery or radiosurgery: a multicenter phase II study
Abstract
Background: Brain metastases reduce survival because therapeutic options are limited. This phase II study evaluated the efficacy of single-agent therapy with alternating weekly, dose-dense temozolomide in pretreated patients with brain metastases prospectively stratified by primary tumor type.
Methods: Eligible patients had bidimensionally measurable brain metastases from histologically/cytologically confirmed melanoma, breast cancer (BC), or non-small-cell lung cancer (NSCLC). Prior chemotherapy, radiotherapy, and whole-brain radiotherapy (WBRT) were allowed. Patients received temozolomide 150 mg/m(2)/day (days 1-7 and 15-21 every 28- or 35-day cycle).
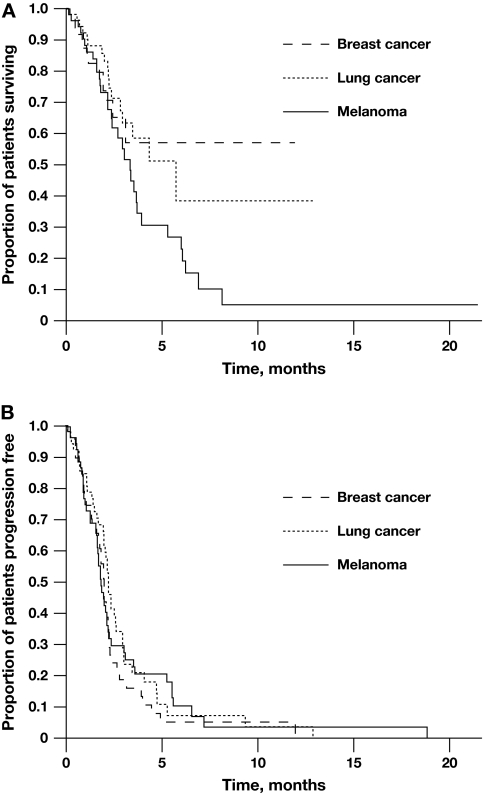
Results: In the intent-to-treat population (N = 157; 53 melanoma, 51 BC, and 53 NSCLC), one patient had complete response, nine (6%) had partial responses, and 31 (20%) had stable disease in the brain. Median progression-free survival was 56, 58, and 66 days for melanoma, BC, and NSCLC, respectively. Median overall survival was 100 days for melanoma, 172 days for NSCLC, and not evaluable in the BC group. Thrombocytopenia was the most common adverse event causing dose modification or treatment discontinuation. Grade 4 toxic effects were rare.
Conclusions: This alternating weekly, dose-dense temozolomide regimen was well tolerated and clinically active in heavily pretreated patients with brain metastases, particularly in patients with melanoma. Combining temozolomide with WBRT or other agents may improve clinical outcomes.
Figures
References
-
- Barnholtz-Sloan JS, Sloan AE, Davis FG, et al. Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. J Clin Oncol. 2004;22:2865–2872. - PubMed
-
- Schouten LJ, Rutten J, Huveneers HA, Twijnstra A. Incidence of brain metastases in a cohort of patients with carcinoma of the breast, colon, kidney, and lung and melanoma. Cancer. 2002;94:2698–2705. - PubMed
-
- Eichler AF, Loeffler JS. Multidisciplinary management of brain metastases. Oncologist. 2007;12:884–898. - PubMed
-
- Lagerwaard FJ, Levendag PC, Nowak PJ, et al. Identification of prognostic factors in patients with brain metastases: a review of 1292 patients. Int J Radiat Oncol Biol Phys. 1999;43:795–803. - PubMed
-
- Gaspar L, Scott C, Rotman M, et al. Recursive partitioning analysis (RPA) of prognostic factors in three Radiation Therapy Oncology Group (RTOG) brain metastases trials. Int J Radiat Oncol Biol Phys. 1997;37:745–751. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
