

ACS-NSQIP has the potential to create an HPB-NSQIP option
- PMID: 19768145
- PMCID: PMC2742610
- DOI: 10.1111/j.1477-2574.2009.00074.x
ACS-NSQIP has the potential to create an HPB-NSQIP option
Abstract
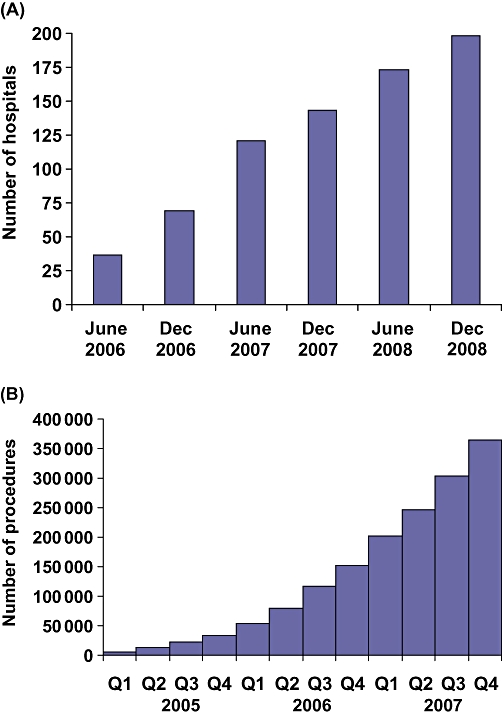
Background: The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) was started in 2004. Presently, 58% of the 198 hospitals participating in ACS-NSQIP are academic or teaching hospitals. In 2008, ACS-NSQIP initiated a number of changes and made risk-adjusted data available for use by participating hospitals. This analysis explores the ACS-NSQIP database for utility in developing hepato-pancreato-biliary (HPB) surgery-specific outcomes (HPB-NSQIP).
Methods: The ACS-NSQIP Participant Use File was queried for patient demographics and outcomes for 49 HPB operations from 1 January 2005 through 31 December 2007. The procedures included six hepatic, 16 pancreatic and 23 complex biliary operations. Four laparoscopic or open cholecystectomy operations were also studied. Risk-adjusted probabilities for morbidity and mortality were compared with observed rates for each operation.
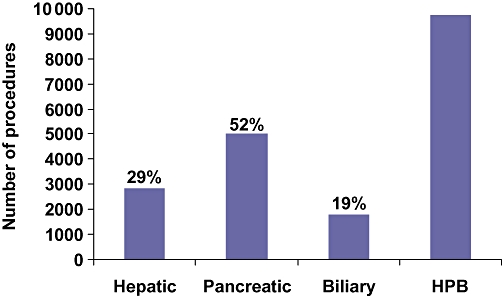
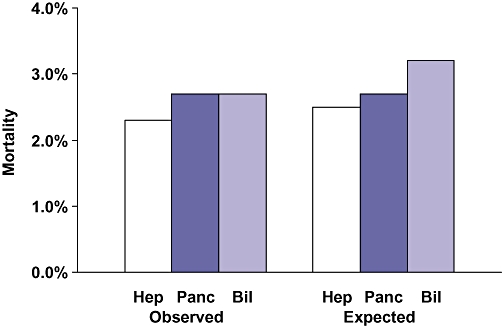
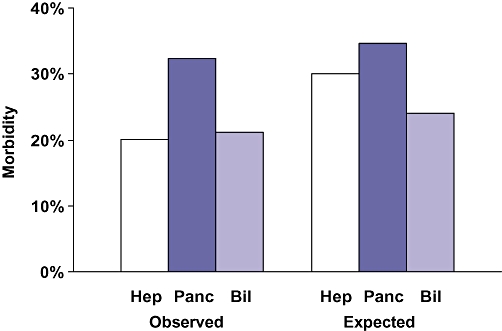
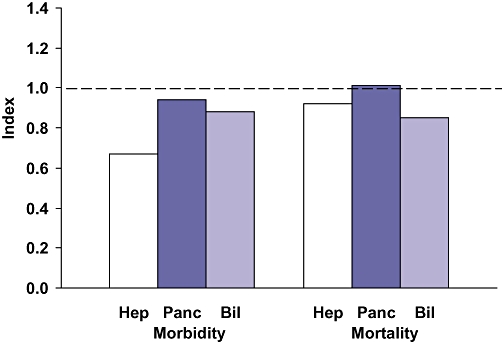
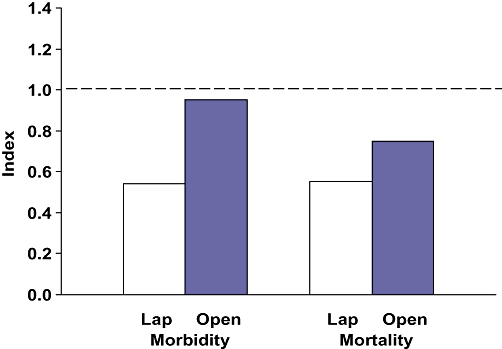
Results: During this 36-month period, data were accumulated on 9723 patients who underwent major HPB surgery, as well as on 44,189 who received cholecystectomies. The major HPB operations included 2847 hepatic (29%), 5074 pancreatic (52%) and 1802 complex biliary (19%) procedures. Patients undergoing hepatic resections were more likely to have metastatic disease (42%) and recent chemotherapy (7%), whereas those undergoing complex biliary procedures were more likely to have significant weight loss (20%), diabetes (13%) and ascites (5%). Morbidity was high for hepatic, pancreatic and complex biliary operations (20.1%, 32.4% and 21.2%, respectively), whereas mortality was low (2.3%, 2.7% and 2.7%, respectively). Compared with laparoscopic cholecystectomy, the open operation was associated with higher rates of morbidity (19.2% vs. 6.0%) and mortality (2.5% vs. 0.3%). The ratios between observed and expected morbidity and mortality rates were <1.0 for hepatic, pancreatic and biliary operations.
Conclusions: These data suggest that HPB operations performed at ACS-NSQIP hospitals have acceptable outcomes. However, the creation of an HPB-NSQIP has the potential to improve quality, provide risk-adjusted registries with HPB-specific data and facilitate multi-institutional clinical trials.
Keywords: cholecystectomy; hepatectomy; hepaticojejunostomy; pancreatectomy; quality.
Figures
References
-
- Khuri SF, Daley J, Henderson WG, Barbour G, Lowry P, Irvin G. The National Veterans Administration Surgical Risk Study: risk adjustment for the comparative assessment of the quality of surgical care. J Am Coll Surg. 1995;180:519–531. - PubMed
-
- Khuri SF, Daley J, Henderson WG, Hur K, Gibbs JO, Barbour G. Risk adjustment of the postoperative mortality rate for the comparative assessment of the quality of surgical care. J Am Coll Surg. 1997;185:315–327. - PubMed
-
- Daley J, Khuri SF, Henderson WG, Hur K, Gibbs JO, Barbour G. Risk adjustment of the postoperative morbidity rate for the comparative assessment of the quality of surgical care. J Am Coll Surg. 1997;185:328–340. - PubMed
-
- Khuri SF, Daley J, Henderson WG, Hur K, Hur K, Demakis J, Aust JB. The Department of Veterans Affairs' NSQIP. The first national, validated, outcome-based, risk-adjusted, and peer-controlled programme for the measurement and enhancement of the quality of surgical care. Ann Surg. 1998;228:491–507. - PMC - PubMed
LinkOut - more resources
Full Text Sources
