

Role of preoperative biliary drainage of liver remnant prior to extended liver resection for hilar cholangiocarcinoma
- PMID: 19768150
- PMCID: PMC2742615
- DOI: 10.1111/j.1477-2574.2009.00090.x
Role of preoperative biliary drainage of liver remnant prior to extended liver resection for hilar cholangiocarcinoma
Abstract
Background: In patients with hilar cholangiocarcinoma, ipsilateral en bloc hepatic resection improves survival but is associated with increased morbidity. Preoperative biliary drainage of the future liver remnant (FLR) and contralateral portal vein embolization (PVE) may improve perioperative outcome, but their routine use is controversial. This study analyses the impact of FLR volume and preoperative biliary drainage on postoperative hepatic insufficiency and mortality rates.
Methods: Patients who underwent hepatic resection and for whom adequate imaging data for FLR calculation were available were identified retrospectively. Patient demographic, operative and perioperative data were recorded and analysed. The volume of the FLR was calculated based on the total liver volume and the volume of the resection that was actually performed using semi-automated contouring of the liver on preoperative helical acquired scans. In patients subjected to preoperative biliary drainage, the preoperative imaging was reviewed to determine if the FLR had been decompressed. Hepatic insufficiency was defined as a postoperative rise in bilirubin of 5 mg/dl above the preoperative level that persisted for >5 days postoperatively. Operative mortality was defined as death related to the operation, whenever it occurred.
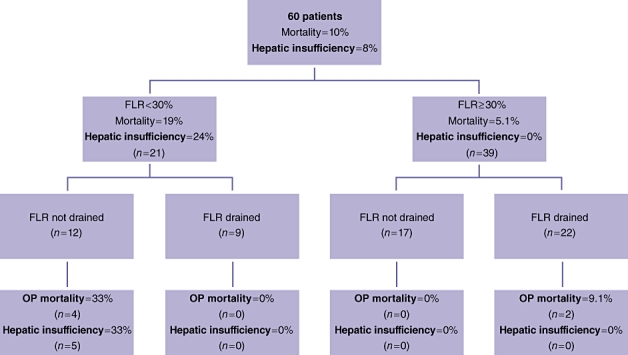
Results: Sixty patients were identified who underwent hepatic resection between 1997 and 2007 and for whom imaging data were available for analysis. During this period, preoperative biliary drainage of the FLR was used selectively and PVE was used in only one patient. The mean age of the patients was 64 +/- 11.6 years and 68% were male. The median length of stay was 14 days and the overall morbidity and mortality were 53% and 10%, respectively. Preoperative FLR volume was a predictor of hepatic insufficiency and death (P= 0.03). A total of 65% of patients had an FLR volume > or = 30% (39/60) of the total volume. No patient in this group had hepatic insufficiency, but there were two operative deaths (5%), both occurring in patients who underwent preoperative biliary drainage. By contrast, in the group with FLR < 30% (21/60, 35%), hepatic insufficiency was seen in five patients and operative mortality in four patients, and were strongly associated with lack of preoperative biliary drainage of the FLR (P = 0.009). Patients with an FLR > or = 30% were more likely to have radiographic evidence of ipsilateral lobar atrophy and hypertrophy of the FLR (46.2% vs. 9.5% in patients with FLR < 30%; P = 0.004).
Conclusions: In patients undergoing liver resection for hilar cholangiocarcinoma, FLR volume of < 30% of total liver volume is associated with increased risk for hepatic insufficiency and death. Preoperative biliary drainage of the FLR appears to improve outcome if the predicted volume is < 30%. However, in patients with FLR > or = 30%, preoperative biliary drainage does not appear to improve perioperative outcome and, as many of these patients have hypertrophy of the FLR, PVE is likely to offer little benefit.
Keywords: biliary drainage; hilar cholangiocarcinoma; jaundice; klatskin tumor.
Figures
References
-
- Launois B, Reding R, Lebeau G, Buard JL. Surgery for hilar cholangiocarcinoma: French experience in a collective survey of 552 extrahepatic bile duct cancers. J Hepatobiliary Pancreat Surg. 2000;7:128–134. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
