

Ventricular scars and ventricular tachycardia
- PMID: 19768192
- PMCID: PMC2744510
Ventricular scars and ventricular tachycardia
Abstract
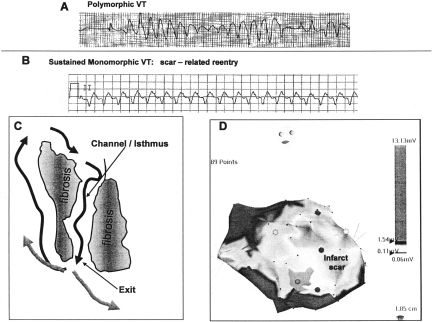
Ventricular tachycardia (VT) is a life-threatening arrhythmia that is common to all forms of heart disease and an important cause of sudden death. Ventricular scars from infarction or replacement fibrosis provide a substrate for reentry that is a common cause. Understanding the pathophysiologic link between ventricular scars and ventricular tachycardia informs approaches to identify patients at risk, has led to development of methods to ablate the arrhythmia substrate that can be applied even in severe heart disease, and suggests future diagnostic and therapeutic strategies.
Conflict of interest statement
Potential Conflicts of Interest:
Figures
References
-
- Stevenson WG, Soejima K. Catheter ablation for ventricular tachycardia. Circulation. 2007;115(21):2750–60. - PubMed
-
- Zeppenfeld K, Schalij MJ, Bartelings MM, Tedrow UB, Koplan BA, Soejima K, Stevenson WG. Catheter ablation of ventricular tachycardia after repair of congenital heart disease: electroanatomic identification of the critical right ventricular isthmus. Circulation. 2007;116(20):2241–52. - PubMed
-
- de Bakker JM, van Capelle FJ, Janse MJ, Tasseron S, Vermeulen JT, de Jonge N, Lahpor JR. Slow conduction in the infarcted human heart. Zigzag course of activation. Circulation. 1993;88(3):915–26. - PubMed
-
- Soejima K, Stevenson WG, Maisel WH, Sapp JL, Epstein LM. Electrically unexcitable scar mapping based on pacing threshold for identification of the reentry circuit isthmus: feasibility for guiding ventricular tachycardia ablation. Circulation. 2002;106(13):1678–83. - PubMed
-
- Poole JE, Johnson GW, Hellkamp AS, Anderson J, Callans DJ, Raitt MH, Reddy RK, Marchlinski FE, Yee R, Guarnieri T, Talajic M, Wilber DJ, Fishbein DP, Packer DL, Mark DB, Lee KL, Bardy GH. Prognostic importance of defibrillator shocks in patients with heart failure. N Engl J Med. 2008;359(10):1009–17. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical