

Microneedle-based vaccines
- PMID: 19768415
- PMCID: PMC2904604
- DOI: 10.1007/978-3-540-92165-3_18
Microneedle-based vaccines
Abstract
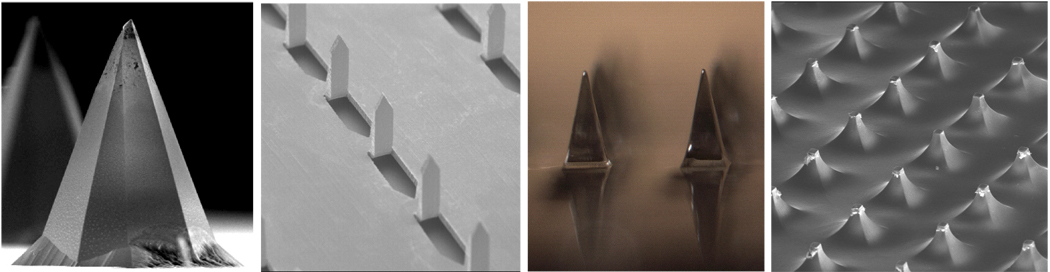
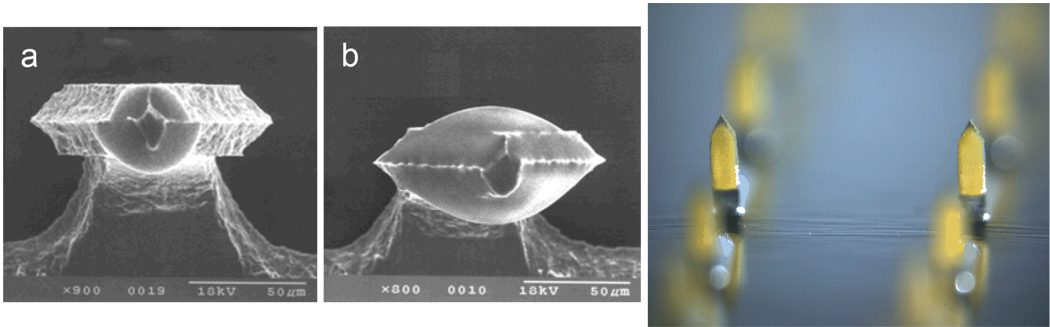
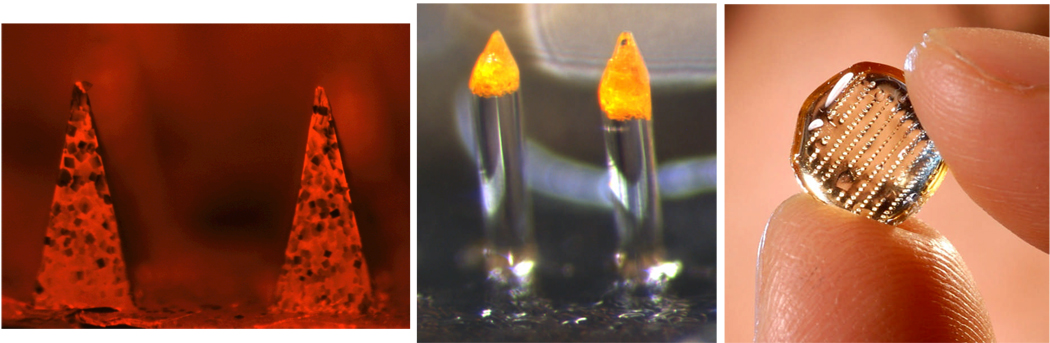
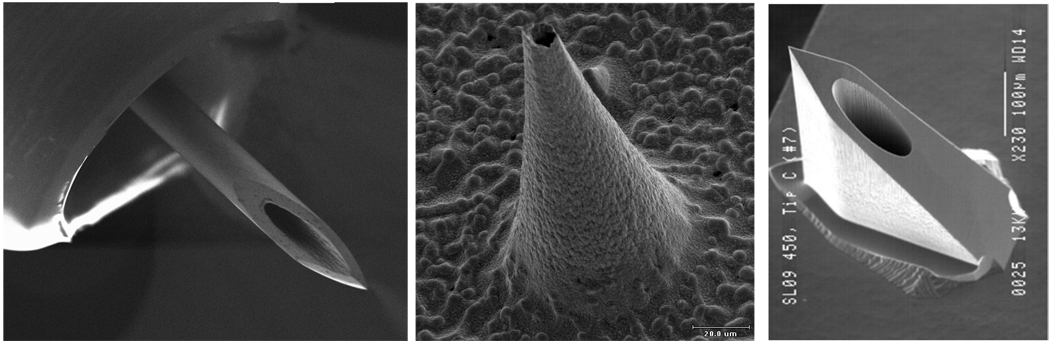
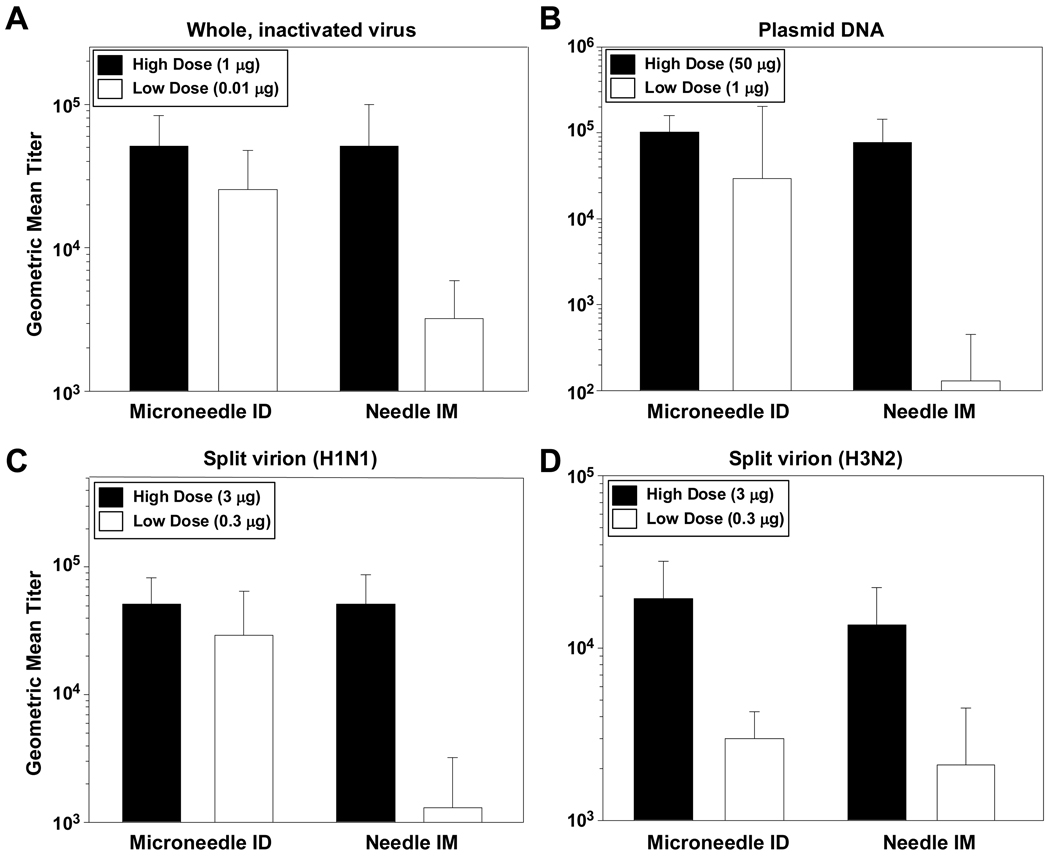
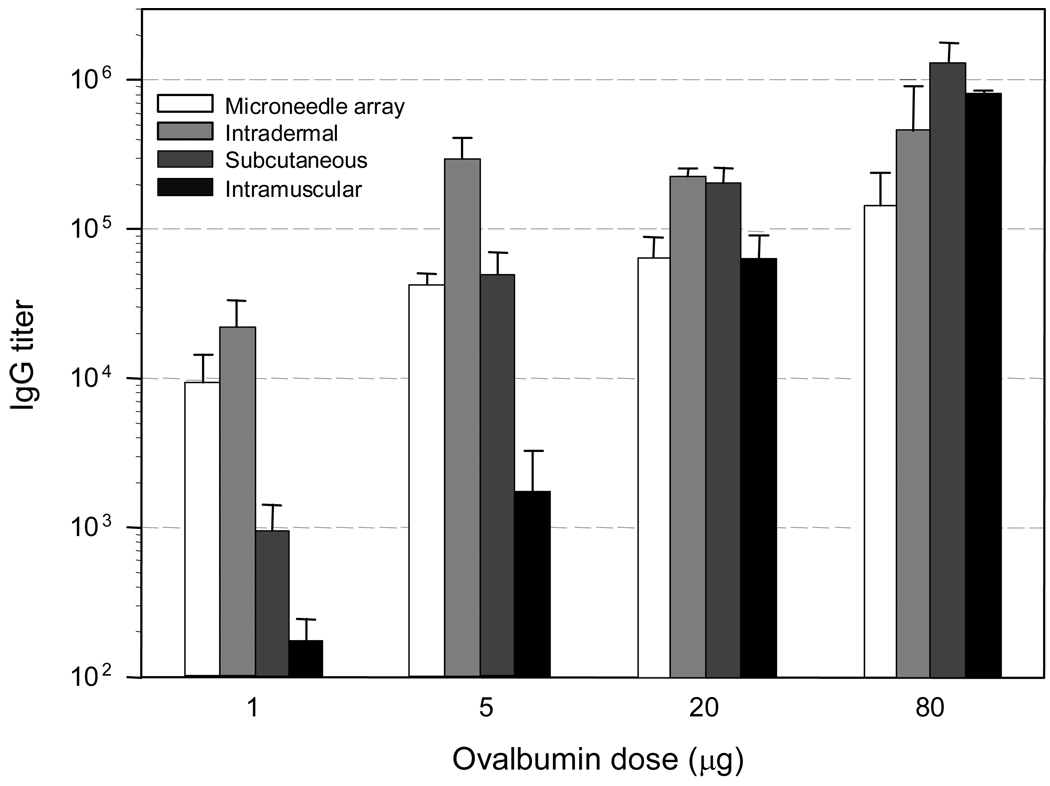
The threat of pandemic influenza and other public health needs motivate the development of better vaccine delivery systems. To address this need, microneedles have been developed as micron-scale needles fabricated using low-cost manufacturing methods that administer vaccine into the skin using a simple device that may be suitable for self-administration. Delivery using solid or hollow microneedles can be accomplished by (1) piercing the skin and then applying a vaccine formulation or patch onto the permeabilized skin, (2) coating or encapsulating vaccine onto or within microneedles for rapid, or delayed, dissolution and release in the skin, and (3) injection into the skin using a modified syringe or pump. Extensive clinical experience with smallpox, TB, and other vaccines has shown that vaccine delivery into the skin using conventional intradermal injection is generally safe and effective and often elicits the same immune responses at lower doses compared to intramuscular injection. Animal experiments using microneedles have shown similar benefits. Microneedles have been used to deliver whole, inactivated virus; trivalent split antigen vaccines; and DNA plasmids encoding the influenza hemagglutinin to rodents, and strong antibody responses were elicited. In addition, ChimeriVax-JE against yellow fever was administered to nonhuman primates by microneedles and generated protective levels of neutralizing antibodies that were more than seven times greater than those obtained with subcutaneous delivery; DNA plasmids encoding hepatitis B surface antigen were administered to mice and antibody and T cell responses at least as strong as hypodermic injections were generated; recombinant protective antigen of Bacillus anthracis was administered to rabbits and provided complete protection from lethal aerosol anthrax spore challenge at a lower dose than intramuscular injection; and DNA plasmids encoding four vaccinia virus genes administered to mice in combination with electroporation generated neutralizing antibodies that apparently included both Th1 and Th2 responses. Dose sparing with microneedles was specifically studied in mice with the model vaccine ovalbumin. At low dose (1 microg), specific antibody titers from microneedles were one order of magnitude greater than subcutaneous injection and two orders of magnitude greater than intramuscular injection. At higher doses, antibody responses increased for all delivery methods. At the highest levels (20-80 microg), the route of administration had no significant effect on the immune response. Concerning safety, no infections or other serious adverse events have been observed in well over 1,000 microneedle insertions in human and animal subjects. Bleeding generally does not occur for short microneedles (<1 mm). Highly localized, mild, and transient erythema is often observed. Microneedle pain has been reported as nonexistent to mild, and always much less than a hypodermic needle control. Overall, these studies suggest that microneedles may provide a safe and effective method of delivering vaccines with the possible added attributes of requiring lower vaccine doses, permitting low-cost manufacturing, and enabling simple distribution and administration.
Figures
References
-
- Physicians' Desk Reference. Montvale, NJ: Thomson PDR; 2007.
-
- Progress toward interruption of wild poliovirus transmission--worldwide, January 2006-May 2007. MMWR Morb Mortal Wkly Rep. 2007;56:682–685. - PubMed
-
- Adams D, Quayum M, Worthington T, Lambert P, Elliott T. Evaluation of a 2% chlorhexidine gluconate in 70% isopropyl alcohol skin disinfectant. J Hosp Infect. 2005;61:287–290. - PubMed
-
- Andersen KE, Boman A, Volund A, Wahlberg JE. Induction of formaldehyde contact sensitivity: dose response relationship in the guinea pig maximization test. Acta Derm Venereol. 1985;65:472–478. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
