

Baseline CSF p-tau levels independently predict progression of hippocampal atrophy in Alzheimer disease
- PMID: 19770469
- PMCID: PMC2839552
- DOI: 10.1212/WNL.0b013e3181b879ac
Baseline CSF p-tau levels independently predict progression of hippocampal atrophy in Alzheimer disease
Abstract
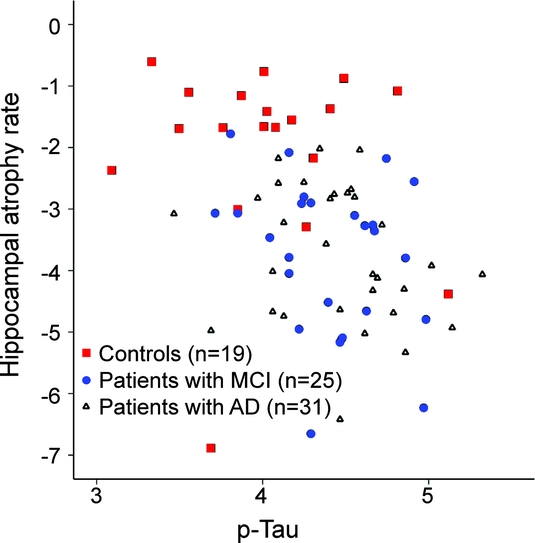
Objective: To investigate whether baseline CSF biomarkers are associated with hippocampal atrophy rate as a measure of disease progression in patients with Alzheimer disease (AD), patients with mild cognitive impairment (MCI), and controls, controlling for baseline neuropsychological and MRI findings.
Methods: We assessed data from 31 patients with AD, 25 patients with MCI, and 19 controls (mean age 68 +/- 8 years; 39 [52%] female) who visited our memory clinic and had received serial MRI scanning (scan interval 1.7 +/- 0.7 years). At baseline, CSF biomarkers (amyloid beta 1-42, tau, and tau phosphorylated at threonine 181 [p-tau]) were obtained, as well as neuropsychological data. Baseline MRI scans were assessed using visual rating scales for medial temporal lobe atrophy (MTA), global cortical atrophy, and white matter hyperintensities. Hippocampal atrophy rates were estimated using regional nonlinear "fluid" registration of follow-up scan to baseline scan.
Results: Stepwise multiple linear regression, adjusted for age and sex, showed that increased CSF p-tau levels (beta [standard error]: -0.79 [0.35]) at baseline was independently associated with higher subsequent hippocampal atrophy rates (p < 0.05), together with poorer memory performance (0.09 [0.04]) and more severe MTA (-0.60 [0.21]). The association of memory function with hippocampal atrophy rate was explained by the link with diagnosis, because it disappeared from the model after we additionally corrected for diagnosis.
Conclusions: Baseline CSF levels of tau phosphorylated at threonine 181 are independently associated with subsequent disease progression, as reflected by hippocampal atrophy rate. This effect is independent of baseline neuropsychological and MRI predictors. Our results imply that predicting disease progression can best be achieved by combining information from different modalities.
Figures
References
-
- Dubois B, Feldman HH, Jacova C, et al. Research criteria for the diagnosis of Alzheimer’s disease: revising the NINCDS-ADRDA criteria. Lancet Neurol 2007;6:734–746. - PubMed
-
- Waldemar G, Dubois B, Emre M, et al. Recommendations for the diagnosis and management of Alzheimer’s disease and other disorders associated with dementia: EFNS guideline. Eur J Neurol 2007;14:e1–e26. - PubMed
-
- McKhann G, Drachman D, Folstein M, et al. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 1984;34:939–944. - PubMed
-
- Guillozet AL, Weintraub S, Mash DC, Mesulam MM. Neurofibrillary tangles, amyloid, and memory in aging and mild cognitive impairment. Arch Neurol 2003;60:729–736. - PubMed
-
- Mortimer JA, Gosche KM, Riley KP, Markesbery WR, Snowdon DA. Delayed recall, hippocampal volume and Alzheimer neuropathology: findings from the Nun Study. Neurology 2004;62:428–432. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical