

Early mortality and cause of deaths in patients using HAART in Brazil and the United States
- PMID: 19770698
- PMCID: PMC3790467
- DOI: 10.1097/QAD.0b013e32832ec494
Early mortality and cause of deaths in patients using HAART in Brazil and the United States
Abstract
Objective: To compare the early mortality pattern and causes of death among patients starting HAART in Brazil and the United States.
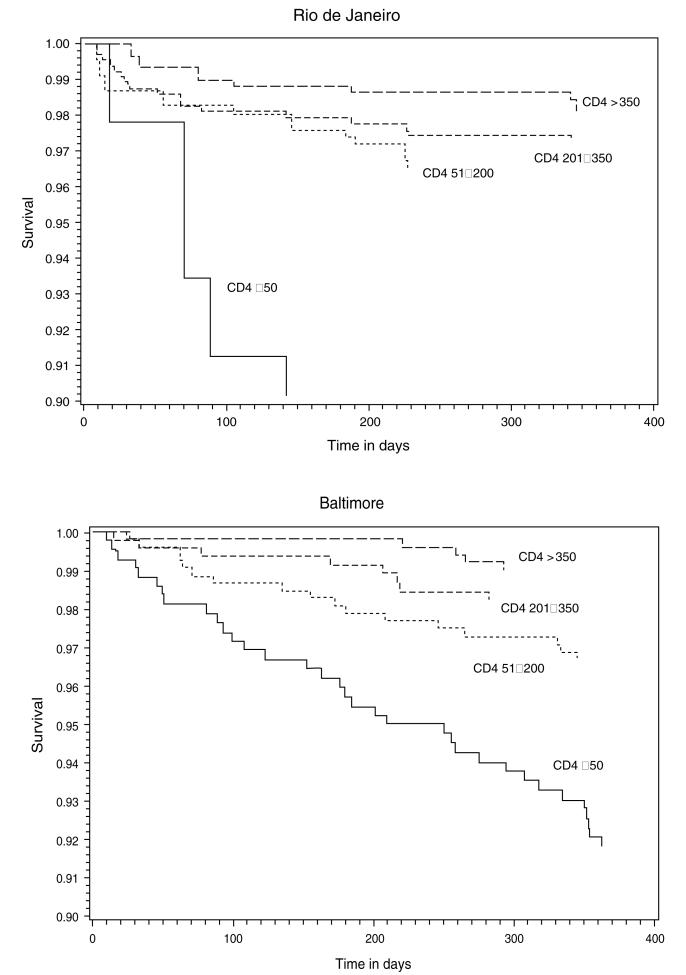
Methods: We analyzed the combined data from two clinical cohorts followed at the Johns Hopkins AIDS Service in Baltimore, United States, and the Evandro Chagas Clinical Research Institute AIDS Clinic in Rio de Janeiro, Brazil. Participants included those who entered either cohort between 1999 and 2007 and were antiretroviral naive. Follow-up was at 1 year since HAART initiation. Cox proportional hazards regression analysis was used to assess the role of the city on the risk of death.
Results: A total of 859 and 915 participants from Baltimore and Rio de Janeiro, respectively, were included. In Rio de Janeiro, 64.7% of deaths occurred within 90 days of HAART initiation; in Baltimore, 48.9% occurred between 180 and 365 days. AIDS-defining illness (61.8%) and non-AIDS-defining illness (55.6%) predominated as causes of death in Rio de Janeiro and Baltimore, respectively. Risk of death was similar in both cities (hazard ratio 1.04; P value = 0.95) after adjusting for CD4 T cell count, age, sex, HIV risk group, prior AIDS-defining illness, and Pneumocystis jirovecii pneumonia and Mycobacterium avium prophylaxis. Individuals with CD4 T cell count less than or equal to 50 cells/microl (hazard ratio 4.36; P = 0.001) or older (hazard ratio, 1.03; P = 0.03) were more likely to die.
Conclusion: Although late HIV diagnosis is a problem both in developed and developing countries, differences in the timing and causes of deaths clearly indicate that, besides interventions for early HIV diagnosis, different strategies to curb early mortality need to be tailored in each country.
Figures
References
-
- Dore GJ, Li Y, McDonald A, Ree H, Kaldor JM. Impact of highly active antiretroviral therapy on individual AIDS-defining illness incidence and survival in Australia. J Acquir Immune Defic Syndr. 2002;29:388–395. - PubMed
-
- Egger M, May M, Chene G, Phillips AN, Ledergerber B, Dabis F, et al. Prognosis of HIV-1-infected patients starting highly active antiretroviral therapy: a collaborative analysis of prospective studies. Lancet. 2002;360:119–129. - PubMed
-
- Hogg RS, Yip B, Chan KJ, Wood E, Craib KJ, O’Shaughnessy MV, Montaner JS. Rates of disease progression by baseline CD4 cell count and viral load after initiating triple-drug therapy. JAMA. 2001;286:2568–2577. - PubMed
-
- Lee LM, Karon JM, Selik R, Neal JJ, Fleming PL. Survival after AIDS diagnosis in adolescents and adults during the treatment era, United States, 1984–1997. JAMA. 2001;285:1308–1315. - PubMed
-
- Braitstein P, Brinkh of MW, Dabis F, Schechter M, Boulle A, Miotti P, et al. Mortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countries. Lancet. 2006;367:817–824. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
