

Biological versus chronological ovarian age: implications for assisted reproductive technology
- PMID: 19772632
- PMCID: PMC2764709
- DOI: 10.1186/1477-7827-7-101
Biological versus chronological ovarian age: implications for assisted reproductive technology
Abstract
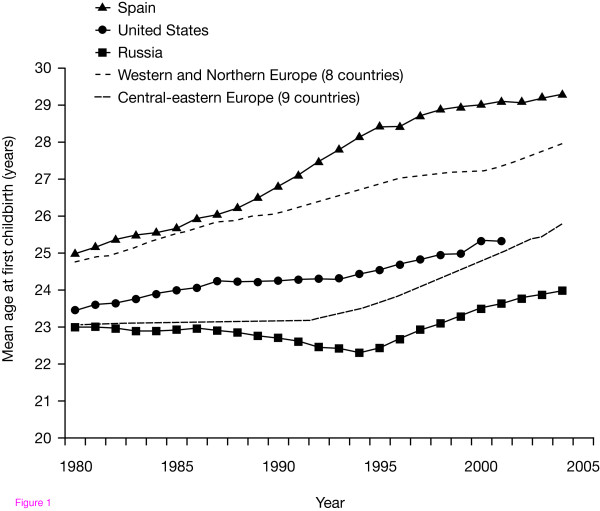
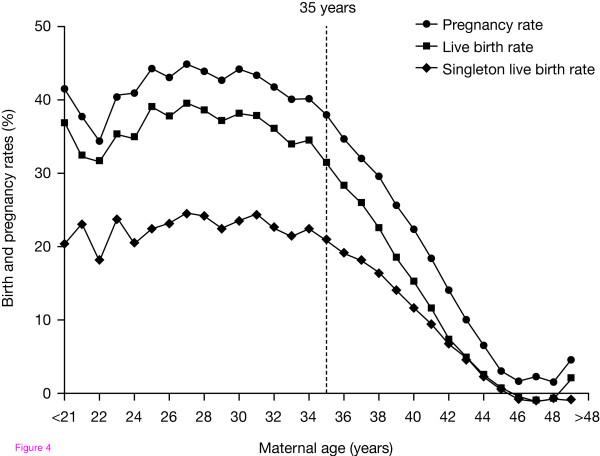
Background: Women have been able to delay childbearing since effective contraception became available in the 1960s. However, fertility decreases with increasing maternal age. A slow but steady decrease in fertility is observed in women aged between 30 and 35 years, which is followed by an accelerated decline among women aged over 35 years. A combination of delayed childbearing and reduced fecundity with increasing age has resulted in an increased number and proportion of women of greater than or equal to 35 years of age seeking assisted reproductive technology (ART) treatment.
Methods: Literature searches supplemented with the authors' knowledge.
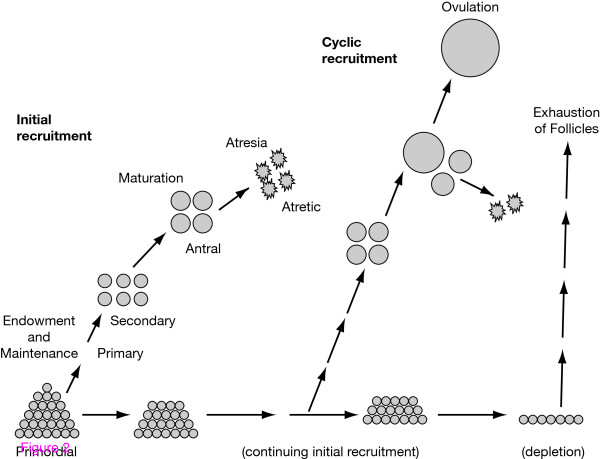
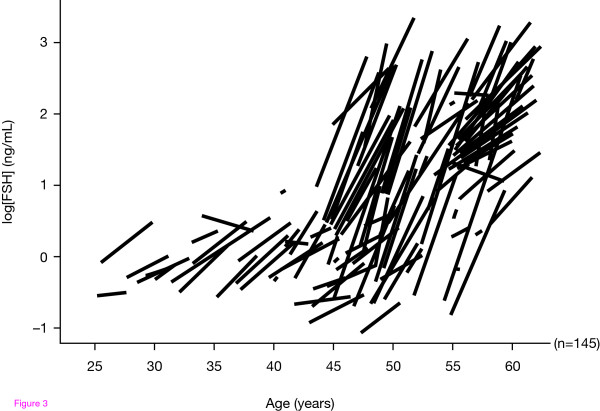
Results: Despite major advances in medical technology, there is currently no ART treatment strategy that can fully compensate for the natural decline in fertility with increasing female age. Although chronological age is the most important predictor of ovarian response to follicle-stimulating hormone, the rate of reproductive ageing and ovarian sensitivity to gonadotrophins varies considerably among individuals. Both environmental and genetic factors contribute to depletion of the ovarian oocyte pool and reduction in oocyte quality. Thus, biological and chronological ovarian age are not always equivalent. Furthermore, biological age is more important than chronological age in predicting the outcome of ART. As older patients present increasingly for ART treatment, it will become more important to critically assess prognosis, counsel appropriately and optimize treatment strategies. Several genetic markers and biomarkers (such as anti-Müllerian hormone and the antral follicle count) are emerging that can identify women with accelerated biological ovarian ageing. Potential strategies for improving ovarian response include the use of luteinizing hormone (LH) and growth hormone (GH). When endogenous LH levels are heavily suppressed by gonadotrophin-releasing hormone analogues, LH supplementation may help to optimize treatment outcomes for women with biologically older ovaries. Exogenous GH may improve oocyte development and counteract the age-related decline of oocyte quality. The effects of GH may be mediated by insulin-like growth factor-I, which works synergistically with follicle-stimulating hormone on granulosa and theca cells.
Conclusion: Patients with biologically older ovaries may benefit from a tailored approach based on individual patient characteristics. Among the most promising adjuvant therapies for improving ART outcomes in women of advanced reproductive age are the administration of exogenous LH or GH.
Figures
Similar articles
-
Advanced reproductive age and fertility.J Obstet Gynaecol Can. 2011 Nov;33(11):1165-1175. doi: 10.1016/S1701-2163(16)35087-3. J Obstet Gynaecol Can. 2011. PMID: 22082792
-
Reproductive potential in the older woman.Fertil Steril. 1986 Dec;46(6):989-1001. doi: 10.1016/s0015-0282(16)49869-9. Fertil Steril. 1986. PMID: 3536609 Review.
-
Ovarian aging and implications for fertility female health.Minerva Endocrinol. 2012 Mar;37(1):41-57. Minerva Endocrinol. 2012. PMID: 22382614 Review.
-
Ovarian aging: mechanisms and clinical consequences.Endocr Rev. 2009 Aug;30(5):465-93. doi: 10.1210/er.2009-0006. Epub 2009 Jul 9. Endocr Rev. 2009. PMID: 19589949 Review.
-
Growth hormone in fertility and infertility: Mechanisms of action and clinical applications.Front Endocrinol (Lausanne). 2022 Nov 14;13:1040503. doi: 10.3389/fendo.2022.1040503. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36452322 Free PMC article. Review.
Cited by
-
GPX3 Overexpression in Cumulus Cells Entails a Poor Prognosis for Uterine Implantation of Morphotype A Embryos.Biology (Basel). 2022 Sep 16;11(9):1361. doi: 10.3390/biology11091361. Biology (Basel). 2022. PMID: 36138840 Free PMC article.
-
The effects and mechanism of taxanes on chemotherapy-associated ovarian damage: A review of current evidence.Front Endocrinol (Lausanne). 2022 Nov 24;13:1025018. doi: 10.3389/fendo.2022.1025018. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36531475 Free PMC article. Review.
-
Female aging alters expression of human cumulus cells genes that are essential for oocyte quality.Biomed Res Int. 2014;2014:964614. doi: 10.1155/2014/964614. Epub 2014 Sep 3. Biomed Res Int. 2014. PMID: 25276836 Free PMC article.
-
The relevance of female overweight in infertility treatment: a position statement of the Italian Society of Fertility and Sterility and Reproductive Medicine (SIFES-MR).J Assist Reprod Genet. 2025 Apr;42(4):1343-1354. doi: 10.1007/s10815-024-03379-0. Epub 2025 Feb 4. J Assist Reprod Genet. 2025. PMID: 39903407 Free PMC article.
-
The role of recombinant LH in ovarian stimulation: what's new?Reprod Biol Endocrinol. 2025 Mar 10;23(Suppl 1):38. doi: 10.1186/s12958-025-01361-8. Reprod Biol Endocrinol. 2025. PMID: 40059197 Free PMC article. Review.
References
-
- Balasch J. Investigation of the infertile couple: investigation of the infertile couple in the era of assisted reproductive technology: a time for reappraisal. Hum Reprod. 2000;15:2251–2257. - PubMed
-
- Leridon H. Can assisted reproduction technology compensate for the natural decline in fertility with age? A model assessment. Hum Reprod. 2004;19:1548–1553. - PubMed
-
- te Velde ER, Pearson PL. The variability of female reproductive ageing. Hum Reprod Update. 2002;8:141–154. - PubMed
-
- Steptoe PC, Edwards RG. Birth after the reimplantation of a human embryo. Lancet. 1978;2:366. - PubMed
-
- Steptoe PC, Edwards RG, Walters DE. Observations on 767 clinical pregnancies and 500 births after human in-vitro fertilization. Hum Reprod. 1986;1:89–94. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
