

Prevalence of osteonecrosis of the jaw in patients with oral bisphosphonate exposure
- PMID: 19772941
- PMCID: PMC10159647
- DOI: 10.1016/j.joms.2009.03.050
Prevalence of osteonecrosis of the jaw in patients with oral bisphosphonate exposure
Abstract
Purpose: Osteonecrosis of the jaw (ONJ) is a serious complication associated with bisphosphonate therapy, but its epidemiology in the setting of oral bisphosphonate therapy is poorly understood. The present study examined the prevalence of ONJ in patients receiving chronic oral bisphosphonate therapy.
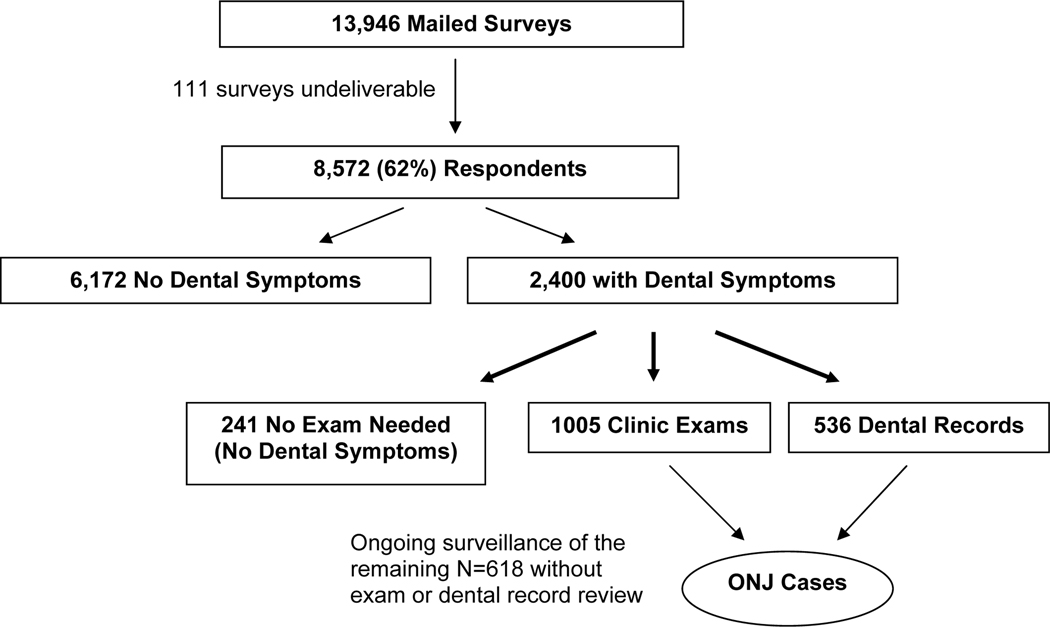
Materials and methods: We mailed a survey to 13,946 members who had received chronic oral bisphosphonate therapy as of 2006 within a large integrated health care delivery system in Northern California. Respondents who reported ONJ, exposed bone or gingival sores, moderate periodontal disease, persistent symptoms, or complications after dental procedures were invited for examination or to have their dental records reviewed. ONJ was defined as exposed bone (of >8 weeks' duration) in the maxillofacial region in the absence of previous radiotherapy.
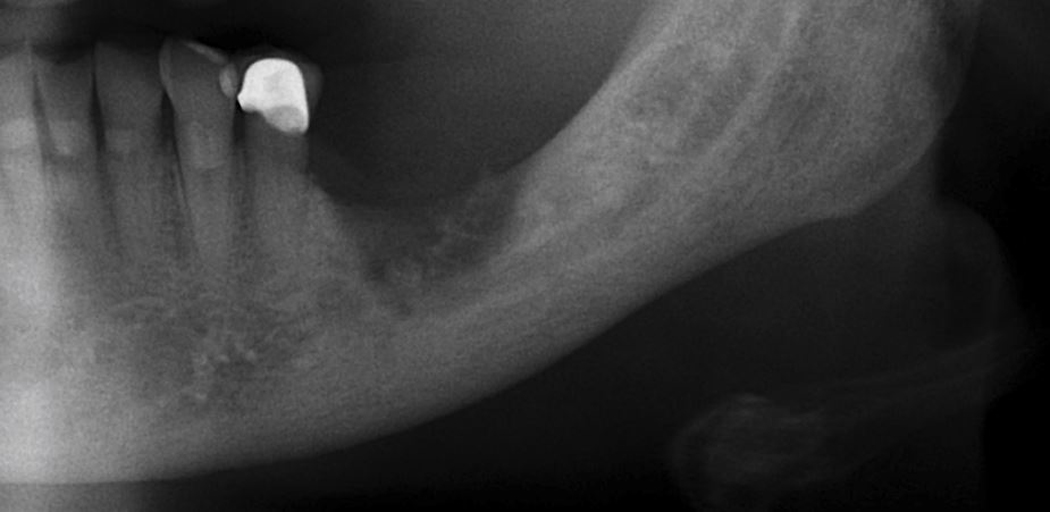
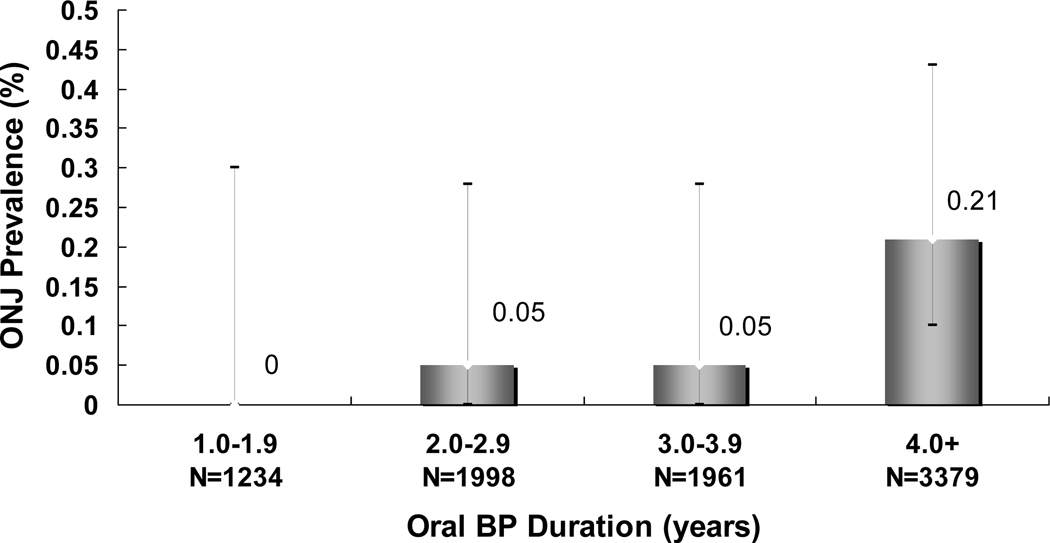
Results: Of the 8,572 survey respondents (71 +/- 9 years, 93% women), 2,159 (25%) reported pertinent dental symptoms. Of these 2,159 patients, 1,005 were examined and an additional 536 provided dental records. Nine ONJ cases were identified, representing a prevalence of 0.10% (95% confidence interval 0.05% to 0.20%) among the survey respondents. Of the 9 cases, 5 had occurred spontaneously (3 in palatal tori) and 4 occurred in previous extraction sites. An additional 3 patients had mandibular osteomyelitis (2 after extraction and 1 with implant failure) but without exposed bone. Finally, 7 other patients had bone exposure that did not fulfill the criteria for ONJ.
Conclusions: ONJ occurred in 1 of 952 survey respondents with oral bisphosphonate exposure (minimum prevalence of 1 in 1,537 of the entire mailed cohort). A similar number had select features concerning for ONJ that did not meet the criteria. The results of the present study provide important data on the spectrum of jaw complications among patients with oral bisphosphonate exposure.
Copyright 2010 American Association of Oral and Maxillofacial Surgeons. All rights reserved.
Figures

References
-
- American Association of Oral and Maxillofacial Surgeons position paper on bisphosphonate-related osteonecrosis of the jaws. J Oral Maxillofac Surg. Mar 2007;65(3):369–376. - PubMed
-
- Marx RE. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic. J Oral Maxillofac Surg. Sep 2003;61(9):1115–1117. - PubMed
-
- Migliorati CA. Bisphosphanates and oral cavity avascular bone necrosis. J Clin Oncol. Nov 15 2003;21(22):4253–4254. - PubMed
-
- Marx RE, Sawatari Y, Fortin M, Broumand V. Bisphosphonate-induced exposed bone (osteonecrosis/osteopetrosis) of the jaws: risk factors, recognition, prevention, and treatment. J Oral Maxillofac Surg. Nov 2005;63(11):1567–1575. - PubMed
-
- Ruggiero SL, Mehrotra B, Rosenberg TJ, Engroff SL. Osteonecrosis of the jaws associated with the use of bisphosphonates: a review of 63 cases. J Oral Maxillofac Surg. May 2004;62(5):527–534. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
