

Comparative analyses of chromosome alterations in soft-tissue metastases within and across patients with castration-resistant prostate cancer
- PMID: 19773449
- PMCID: PMC2771763
- DOI: 10.1158/0008-5472.CAN-08-3810
Comparative analyses of chromosome alterations in soft-tissue metastases within and across patients with castration-resistant prostate cancer
Abstract
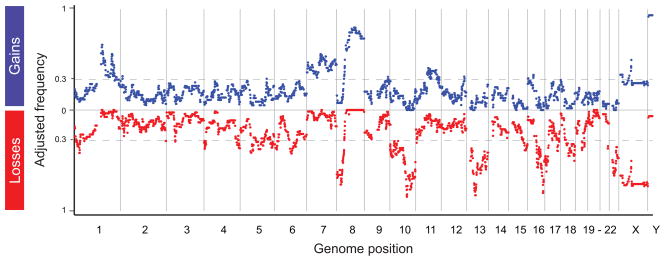
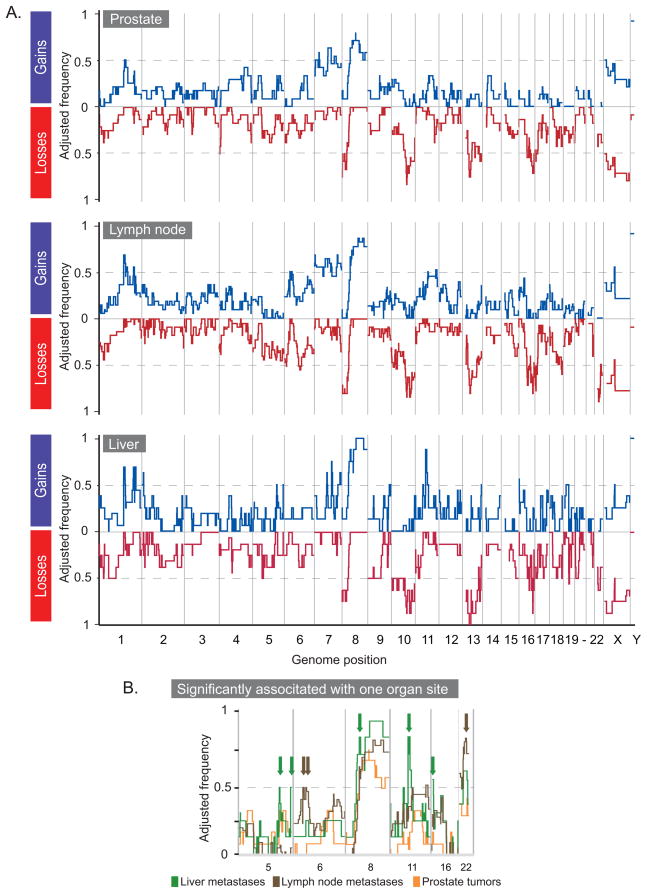
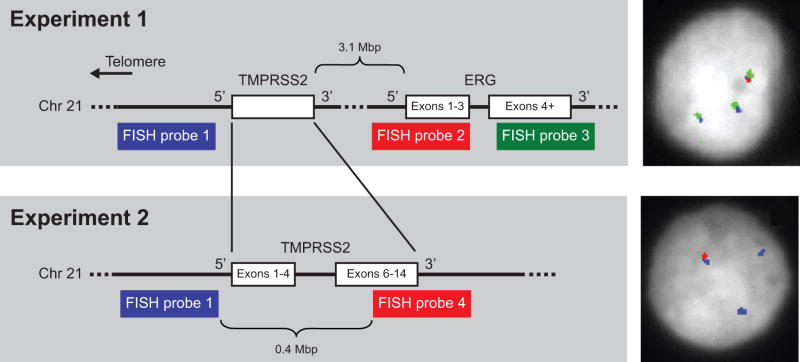
Androgen deprivation is the mainstay of therapy for progressive prostate cancer. Despite initial and dramatic tumor inhibition, most men eventually fail therapy and die of metastatic castration-resistant (CR) disease. Here, we characterize the profound degree of genomic alteration found in CR tumors using array comparative genomic hybridization (array CGH), gene expression arrays, and fluorescence in situ hybridization (FISH). Bycluster analysis, we show that the similarity of the genomic profiles from primary and metastatic tumors is driven by the patient. Using data adjusted for this similarity, we identify numerous high-frequency alterations in the CR tumors, such as 8p loss and chromosome 7 and 8q gain. By integrating array CGH and expression array data, we reveal genes whose correlated values suggest they are relevant to prostate cancer biology. We find alterations that are significantly associated with the metastases of specific organ sites, and others with CR tumors versus the tumors of patients with localized prostate cancer not treated with androgen deprivation. Within the high-frequency sites of loss in CR metastases, we find an overrepresentation of genes involved in cellular lipid metabolism, including PTEN. Finally, using FISH, we verify the presence of a gene fusion between TMPRSS2 and ERG suggested by chromosome 21 deletions detected by array CGH. We find the fusion in 54% of our CR tumors, and 81% of the fusion-positive tumors contain cells with multiple copies of the fusion. Our investigation lays the foundation for a better understanding of and possible therapeutic targets for CR disease, the poorly responsive and final stage of prostate cancer.
Figures

References
-
- Garmey EG, Sartor O, Halabi S, Vogelzang NJ. Second-line chemotherapy for advanced hormone-refractory prostate cancer. Clin Adv Hematol Oncol. 2008;6:118–22. 27–32. - PubMed
-
- Dreicer R. Current status of cytotoxic chemotherapy in patients with metastatic prostate cancer. Urol Oncol. 2008;26:426–9. - PubMed
-
- Ahlers CM, Figg WD. ETS-TMPRSS2 fusion gene products in prostate cancer. Cancer Biol Ther. 2006;5:254–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01DC004209/DC/NIDCD NIH HHS/United States
- R01 GM07365/GM/NIGMS NIH HHS/United States
- R01 CA098415/CA/NCI NIH HHS/United States
- P50 CA097186/CA/NCI NIH HHS/United States
- U24 CA080295/CA/NCI NIH HHS/United States
- R01 DC004209/DC/NIDCD NIH HHS/United States
- T32 HG000035/HG/NHGRI NIH HHS/United States
- U24 CA80295/CA/NCI NIH HHS/United States
- P01 CA085859/CA/NCI NIH HHS/United States
- R01 DK069690/DK/NIDDK NIH HHS/United States
- T32 HG00035/HG/NHGRI NIH HHS/United States
- R01CA098415/CA/NCI NIH HHS/United States
- R01 CA95717/CA/NCI NIH HHS/United States
- R01 CA095717/CA/NCI NIH HHS/United States
- T32 GM007365/GM/NIGMS NIH HHS/United States
- CA97186/CA/NCI NIH HHS/United States
- R01 AG014358/AG/NIA NIH HHS/United States
- R01 AG14358/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
