

Pictorial essay: MRI of the fetal brain
- PMID: 19774144
- PMCID: PMC2747421
- DOI: 10.4103/0971-3026.45349
Pictorial essay: MRI of the fetal brain
Abstract
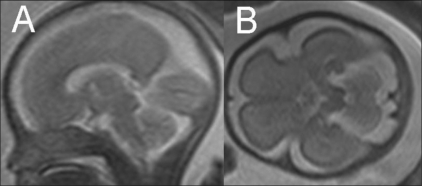
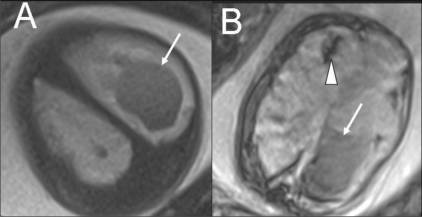
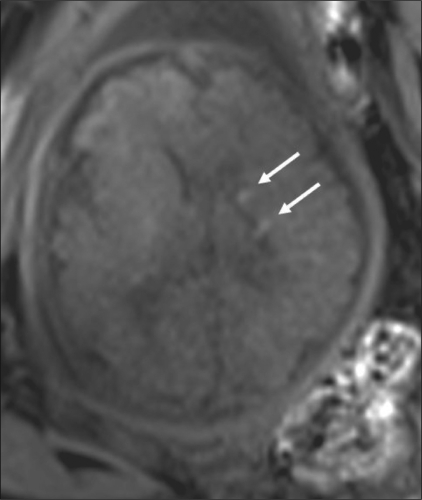
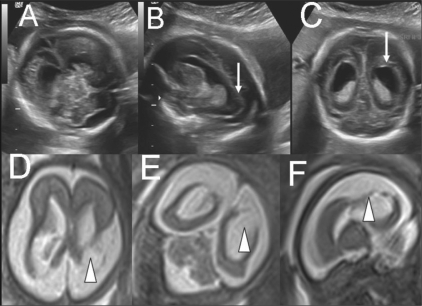
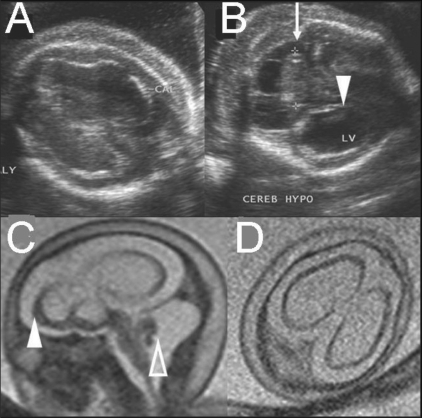
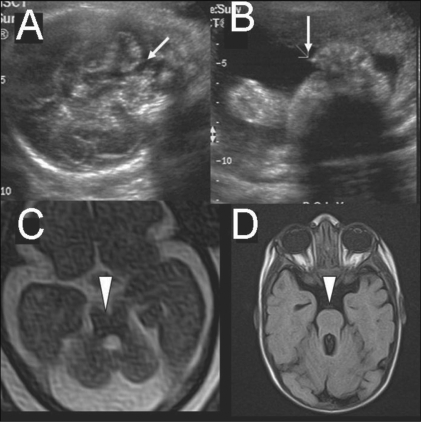
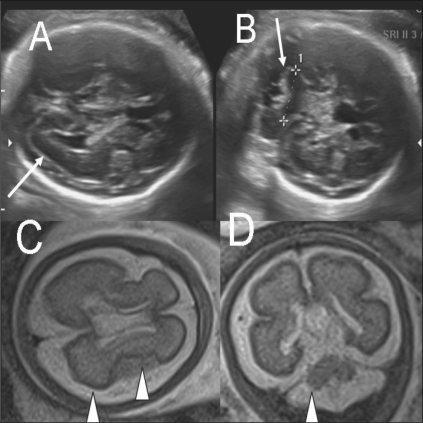
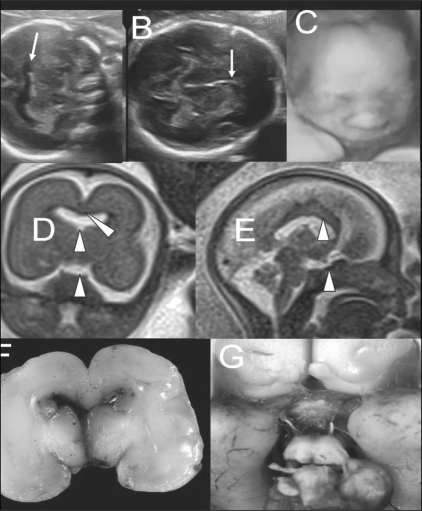
MRI is a useful supplement to USG for the assessment of fetal brain malformations. Superior soft tissue contrast and the ability to depict sulcation and myelination are the strengths of MRI. Subtle or inconclusive USG abnormalities can be confirmed or ruled out by MRI. In some cases, additional findings detected with MRI often help in arriving at a definitive diagnosis, which is necessary for parental counseling and for guiding management. Fast T2W sequences form the basis of fetal MRI. There have been no reports of deleterious effects of MRI on the fetus. A few case examples are presented to illustrate the advantages of MRI.
Keywords: Brain; MRI; fetal.
Conflict of interest statement
Figures

Similar articles
-
Fetal MRI: A pictorial essay.Indian J Radiol Imaging. 2016 Jan-Mar;26(1):52-62. doi: 10.4103/0971-3026.178326. Indian J Radiol Imaging. 2016. PMID: 27081224 Free PMC article.
-
Fetal magnetic resonance imaging of the central nervous system: a pictorial essay.Eur Radiol. 2002 Aug;12(8):1952-61. doi: 10.1007/s00330-001-1281-2. Epub 2002 Feb 2. Eur Radiol. 2002. PMID: 12136313 Review.
-
Extrafetal Findings on Fetal Magnetic Resonance Imaging: A Pictorial Essay.Semin Ultrasound CT MR. 2015 Dec;36(6):550-67. doi: 10.1053/j.sult.2015.07.001. Epub 2015 Jul 31. Semin Ultrasound CT MR. 2015. PMID: 26614136 Review.
-
MRI of fetal abdominal abnormalities.Abdom Imaging. 2003 Nov-Dec;28(6):877-86. doi: 10.1007/s00261-003-0047-5. Abdom Imaging. 2003. PMID: 14753611
-
Fetal magnetic resonance imaging in obstetric practice.J Turk Ger Gynecol Assoc. 2011 Mar 1;12(1):39-46. doi: 10.5152/jtgga.2011.09. eCollection 2011. J Turk Ger Gynecol Assoc. 2011. PMID: 24591956 Free PMC article. Review.
References
-
- Levine D, Barnes D, Madsen JR, Li W, Edelman RR. Fetal central nervous system anomalies: MR imaging augments sonographic diagnosis. Radiology. 1997;204:35–64. - PubMed
-
- Coakley FV, Glenn OA, Qayyum A, Barkovich AJ, Golstein R, Filly RA. Fetal MRI: A developing technique for the developing patient. AJR Am J Roentgenol. 2004;182:242–53,55. - PubMed
-
- Twickler DM, Magee KP, Caire J, Zaretsky M, Fleckenstein JL, Ramus RM. Second-opinion magnestic resonance imaging for suspected fetal central nervous system abnormalities. Am J Obstet Gynecol. 2003;188:492–6. - PubMed
-
- Sonigo C, Rypens FF, Carteret M, Delezoide AL, Brunelle FO. MR imaging of fetal cerebral anomalies. Pediatr Radiol. 1998;28:212–22. - PubMed
-
- Garel C. Berlin: Springer; 2004. MRI of the Fetal Brain; p. 267.
LinkOut - more resources
Full Text Sources