

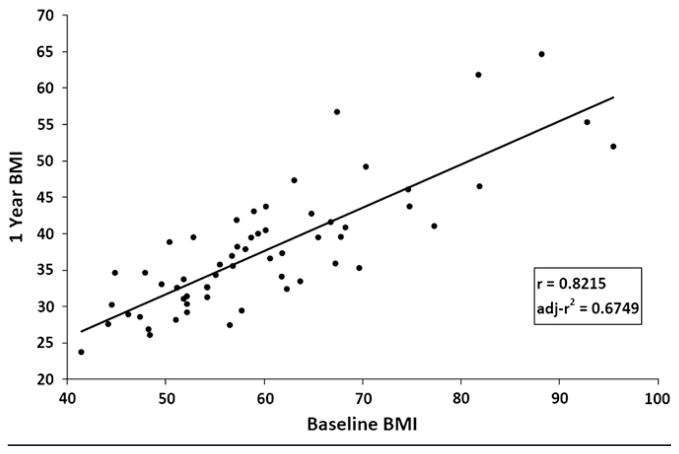
Baseline BMI is a strong predictor of nadir BMI after adolescent gastric bypass
- PMID: 19775700
- PMCID: PMC2886665
- DOI: 10.1016/j.jpeds.2009.07.028
Baseline BMI is a strong predictor of nadir BMI after adolescent gastric bypass
Abstract
Objective: Surgical treatment of extreme obesity may be appropriate for some adolescents. We hypothesized that surgical weight loss outcomes may differ by preoperative level of extreme obesity (body mass index [BMI] > or=99th percentile).
Study design: A longitudinal assessment of clinical characteristics from 61 adolescents who underwent laparoscopic Roux-en-Y gastric bypass at a single pediatric center from 2002 until 2007 was performed. Patients were categorized into 1 of 3 preoperative BMI groups: group 1, BMI = 40.0 to 54.9 (n = 23); group 2, BMI = 55.0 to 64.9 (n = 21); group 3, BMI = 65.0 to 95.0 (n = 17). Changes in BMI and cardiovascular risk factors between baseline and year 1 were evaluated using repeated-measures mixed linear modeling.
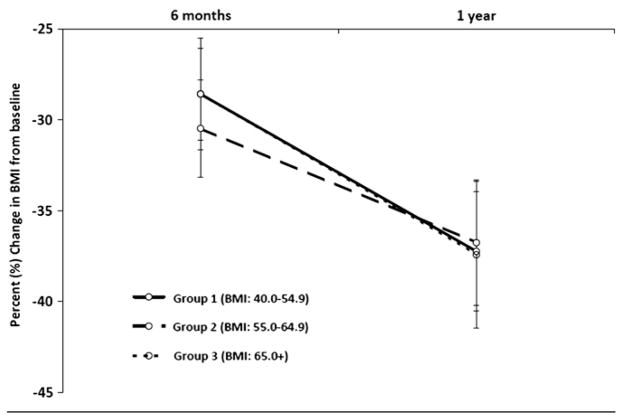
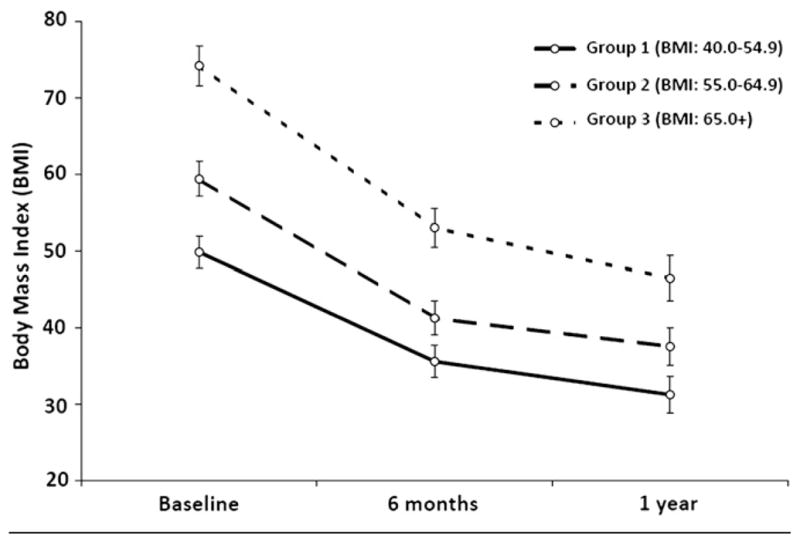
Results: BMI in the overall cohort at baseline (60.2 +/- 11 kg/m(2)) decreased by 37.4% at 1 year after surgery (P < .001). Percent BMI change varied little by preoperative BMI groups (-37.2%, -36.8%, and -37.7% for groups 1, 2, and 3 respectively; P = .8762). The rate of change in absolute BMI units significantly varied by preoperative BMI class (group x time interaction, P < .0001), with 1-year nadir BMI values for groups 1, 2, and 3 falling to 31 +/- 4 kg/m(2), 38 +/- 5 kg/m(2), and 47 +/- 9 kg/m(2), respectively. One year after surgery, only 17% of patients achieved a nonobese BMI (<30 kg/m(2)). Significant improvements in systolic and diastolic blood pressure (P < .0001), fasting insulin (P < .0001), total cholesterol (P = .0007), and triglyceride levels (P < .0001) were seen after surgery irrespective of baseline BMI class. Mean albumin levels remained normal despite significant caloric restriction and weight loss.
Conclusions: Laparoscopic gastric bypass resulted in improvement or reversal of cardiovascular risk factors and resulted in a decrease in BMI of approximately 37% in all patients, regardless of starting BMI, 1 year after surgery. The timing of surgery for adolescent extreme obesity is an important consideration, because "late" referral for bariatric surgery at the highest of BMI values may preclude reversal of obesity.
Figures
References
-
- Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. Prevalence of overweight and obesity in the United States, 1999–2004. JAMA. 2006;295:1549–55. - PubMed
-
- Sturm R. Increases in clinically severe obesity in the United States, 1986–2000. Arch Intern Med. 2003;163:2146–8. - PubMed
-
- Pinhas-Hamiel O, Dolan LM, Daniels SR, Standiford D, Khoury PR, Zeitler P. Increased incidence of non-insulin-dependent diabetes mellitus among adolescents. J Pediatr. 1996;128:608–15. - PubMed
-
- Weiss R, Dziura J, Burgert TS, Tamborlane WV, Taksali SE, Yeckel CW, et al. Obesity and the metabolic syndrome in children and adolescents. N Engl J Med. 2004;350:2362–74. - PubMed
-
- Silvestri JM, Weese-Mayer DE, Bass MT, Kenny AS, Hauptman SA, Pearsall SM. Polysomnography in obese children with a history of sleep-associated breathing disorders. Pediatr Pulmonol. 1993;16:124–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
