

Osteotomy around young deformed knees: 38-year super-long-term follow-up to detect osteoarthritis
- PMID: 19777231
- PMCID: PMC2899361
- DOI: 10.1007/s00264-009-0873-3
Osteotomy around young deformed knees: 38-year super-long-term follow-up to detect osteoarthritis
Abstract
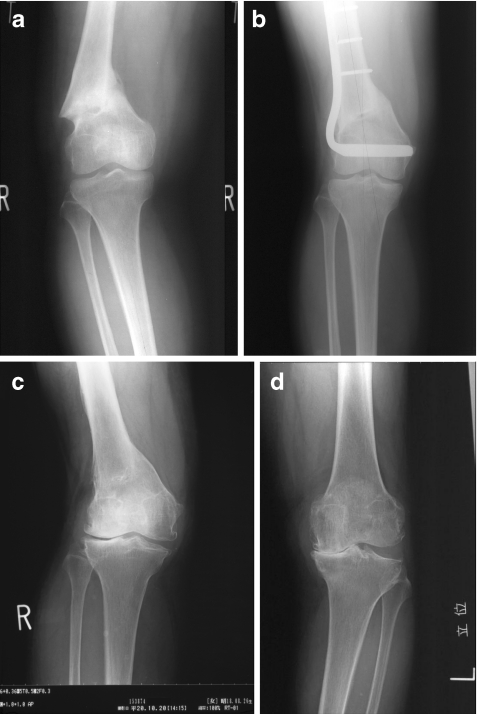
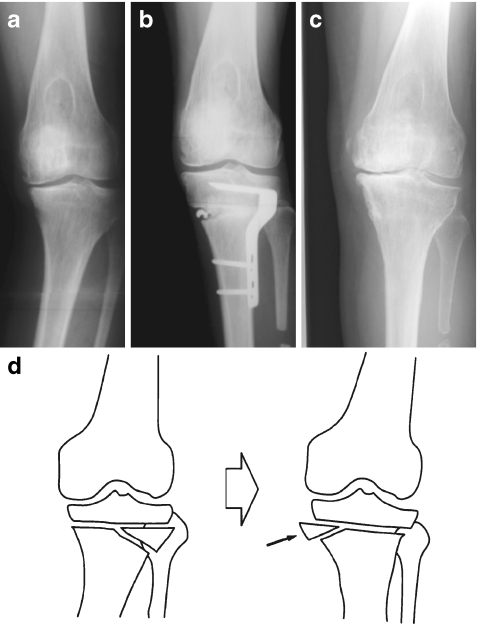
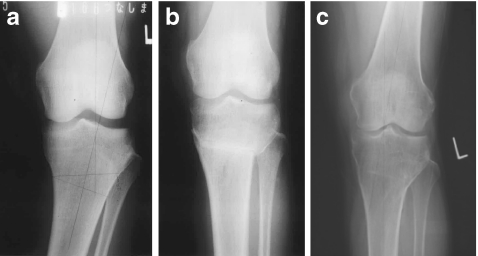
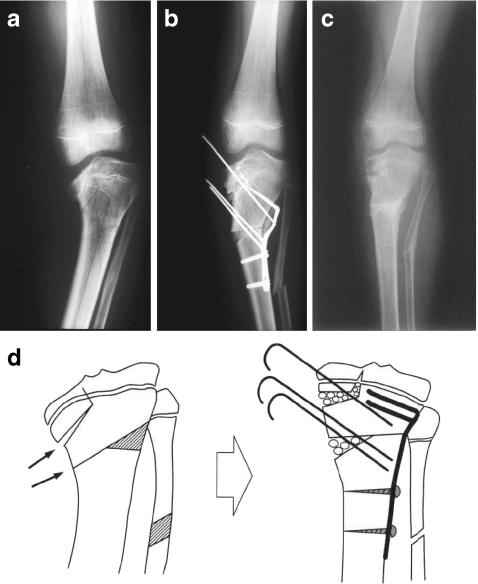
Since 1969 corrective osteotomy has been performed at our institute in young patients (under 40 years) with bowlegs, knock knees and flexion or rotational deformities around the knee. Fifty-seven knees (29 left, 28 right) of 45 patients (19 boys, 26 girls) were followed-up for a period ranging from 30 to 38 years in seven patients with seven knees, from 20 to 29 years in nine patients with 11 knees, and from ten to 19 years in 29 patients with 39 knees. Supracondylar femoral osteotomy was performed on 12 knees (11 patients), high tibial osteotomy above the tibial tuberosity on eight knees (six patients) and below the tuberosity on 37 knees (28 patients). At the final follow-up (age range 42-73 years), all of the deformities were satisfactorily corrected, with no symptoms apart from nine knees, seven of which had dull pain after strenuous sport with osteophytes, etc. in the radiograph. Total knee arthroplasty was performed in the remaining two knees, at ten and 26 years, respectively, after the initial osteotomy. Osteoarthritis developed in the contralateral knee to the initial osteotomy in two patients after 34 years at age 73 and after 33 years at age 67.
Figures
References
-
- Aglietti P, Rinonapoli E, Stringa G, et al. Tibial osteotomy for the varus osteoarthritic knee. Clin Orthop. 1983;176:239–251. - PubMed
-
- Bauer GCH, Insall JN, Koshino T. Tibial osteotomy in gonarthrosis (osteoarthritis of the knee) J Bone Joint Surg. 1969;51-A:1545–1563. - PubMed
-
- Billings A, Scott DF, Camargo MP, et al. High tibial osteotomy with a calibrated osteotomy guide, rigid internal fixation, and early motion. Long-term follow-up. J Bone Joint Surg. 2000;82-A:70–79. - PubMed
-
- Coventry MB, Ilstrup DM, Wallrich SL. Proximal tibial osteotomy – a critical long-term study of eighty-seven cases. J Bone Joint Surg. 1993;75A:196–201. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
