

Phase III, randomised, multicentre trial of maintenance immunotherapy with low-dose interleukin-2 and interferon-alpha for metastatic renal cell cancer
- PMID: 19779715
- PMCID: PMC11031053
- DOI: 10.1007/s00262-009-0773-9
Phase III, randomised, multicentre trial of maintenance immunotherapy with low-dose interleukin-2 and interferon-alpha for metastatic renal cell cancer
Abstract
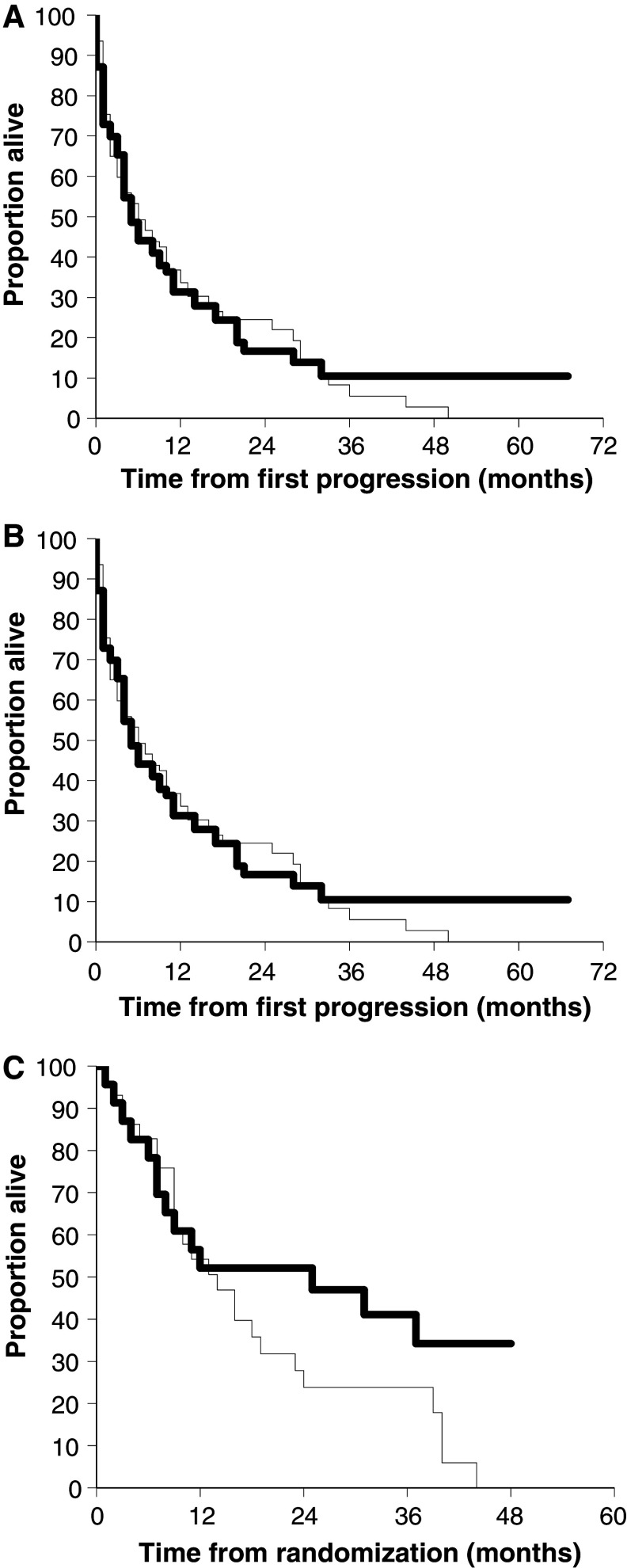
This is the first phase III randomised trial to evaluate maintenance immunotherapy in metastatic renal cell cancer (mRCC). Patients were randomised to receive treatment with a 4-week cycle of subcutaneous low doses IL-2 + IFN in months 1, 3 and 5, and then every 3 months until the first documented disease progression (arm A, suspension), or the same regimen, with chronic maintenance of immunotherapy, regardless of tumour response, until death or intolerable toxicity (arm B, maintenance). The primary endpoint was overall survival (OS); secondary endpoints were time from first progression to death (TFPTD) and tolerability. One hundred and eighty-three patients were enrolled between January 1998 and November 2003. After a median follow-up of 53.9 months, response rate, median OS and median TFPTD were 14.7% (6.3% CR) versus 11.3% (5.5% CR), 14 versus 14 months, 6 versus 5 months, in arms A and B, respectively with no significant differences between the groups. Cox regression analysis showed that the use of chemotherapy after first progression (HR 0.54; 95% CI 0.35-0.86; p = 0.008), PS = 0 (HR 0.53; 95% CI 0.35-0.81; p = 0.001) and female gender (HR 0.63; 95% CI 0.41-0.98; p = 0.038) were significantly associated with a longer TFPTD; treatment arm was not significant (HR 0.88; 95% CI 0.60-1.31; p = 0.54). Toxicity was mainly limited to WHO grades 1 or 2. Chronic maintenance immunotherapy after disease progression is feasible, but does not significantly increase OS or the TFPTD.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
