

Enhanced recovery after surgery (ERAS) versus conventional postoperative care in colorectal surgery
- PMID: 19779947
- PMCID: PMC2793377
- DOI: 10.1007/s11605-009-1037-x
Enhanced recovery after surgery (ERAS) versus conventional postoperative care in colorectal surgery
Abstract
Background: Enhanced Recovery After Surgery (ERAS) programs are associated with reduced hospital morbidity and mortality. The aim of the present study was to evaluate whether the introduction of ERAS care improved the adverse events in colorectal surgery. In a cohort study, mortality, morbidity, and length of stay were compared between ERAS patients and carefully matched historical controls.
Methods: Patients were matched for their type of disease, the type of surgery, P-Possum (Portsmouth-Possum), CR-Possum (Colorectal-Possum) Physiological and Operative Score for Enumeration of Mortality and Morbidity (POSSUM), gender, and American Society of Anesthesiologists (ASA) grade. The primary outcome measures of this study were mortality and morbidity. Secondary outcome measures were fluid intake, length of hospital stay, the number of relaparotomies, and the number of readmissions within 30 days. Data on the ERAS patients were collected prospectively.
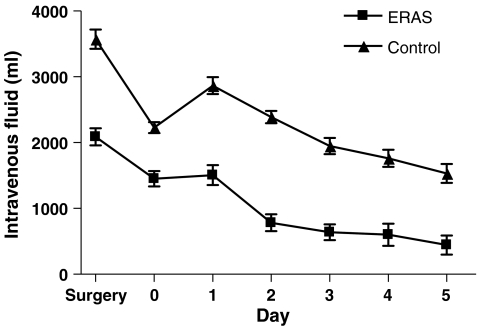
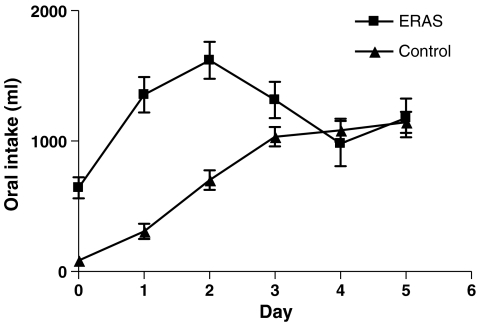
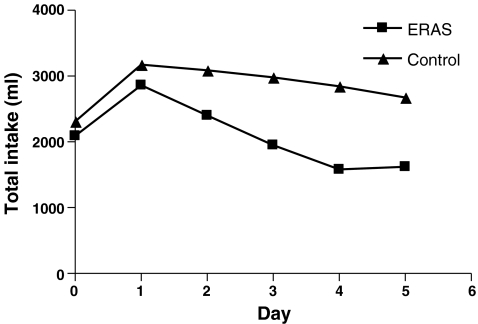
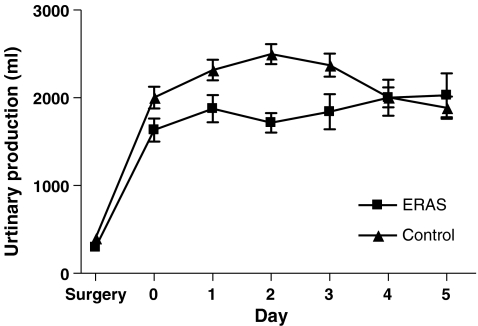
Results: Sixty-one patients treated according to the ERAS program were compared with 122 patients who received conventional postoperative care. The two groups were comparable with respect to age, ASA grade, P-Possum (Portsmouth-Possum), CR-Possum (Colorectal-Possum) score, type of surgery, stoma formation, type of disease, and gender. Morbidity was lower in the ERAS group compared to the control group (14.8% versus 33.6% respectively; P = <0.01). Patients in the ERAS group received significantly less fluid and spent fewer days in the hospital (median 6 days, range 3-50 vs. median 9 days, range 3-138; P = 0.032). There was no difference between the ERAS and the control group for mortality (0% vs. 1.6%; P = 0.55) and readmission rate (3.3% vs. 1.6%; P = 0.60).
Conclusion: Enhanced Recovery After Surgery program reduces morbidity and the length of hospital stay for patients undergoing elective colonic or rectal surgery.
Figures
References
-
- Zargar-Shoshtari K, Hill AG. Optimization of perioperative care for colonic surgery: a review of the evidence. ANZ J Surg. 2008;78(1–2):13–23. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
