

Hepatic wound repair
- PMID: 19781064
- PMCID: PMC2760508
- DOI: 10.1186/1755-1536-2-4
Hepatic wound repair
Abstract
Background: Human chronic liver diseases (CLDs) with different aetiologies rely on chronic activation of wound healing that represents the driving force for fibrogenesis progression (throughout defined patterns of fibrosis) to the end stage of cirrhosis and liver failure.
Issues: Fibrogenesis progression has a major worldwide clinical impact due to the high number of patients affected by CLDs, increasing mortality rate, incidence of hepatocellular carcinoma and shortage of organ donors for liver transplantation.
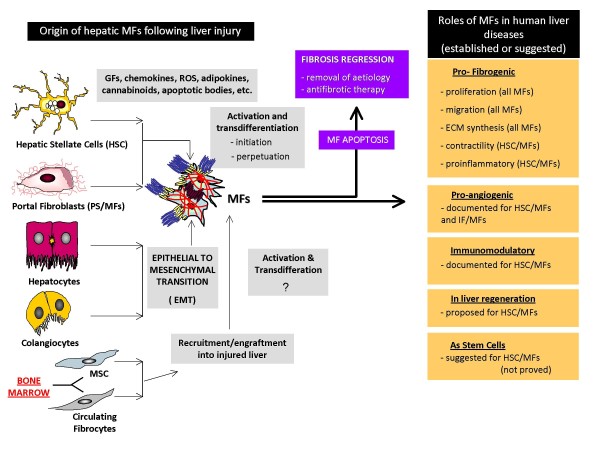
Basic science advances: Liver fibrogenesis is sustained by a heterogeneous population of profibrogenic hepatic myofibroblasts (MFs), the majority being positive for alpha smooth muscle actin (alphaSMA), that may originate from hepatic stellate cells and portal fibroblasts following a process of activation or from bone marrow-derived cells recruited to damaged liver and, in a method still disputed, by a process of epithelial to mesenchymal transition (EMT) involving cholangiocytes and hepatocytes. Recent experimental and clinical data have identified, at tissue, cellular and molecular level major profibrogenic mechanisms: (a) chronic activation of the wound-healing reaction, (b) oxidative stress and related reactive intermediates, and (c) derangement of epithelial-mesenchymal interactions. CLINICAL CARE RELEVANCE: Liver fibrosis may regress following specific therapeutic interventions able to downstage or, at least, stabilise fibrosis. In cirrhotic patients, this would lead to a reduction of portal hypertension and of the consequent clinical complications and to an overall improvement of liver function, thus extending the complication-free patient survival time and reducing the need for liver transplantation.
Conclusion: Emerging mechanisms and concepts related to liver fibrogenesis may significantly contribute to clinical management of patients affected by CLDs.
Figures
References
LinkOut - more resources
Full Text Sources
