

Identification of early interstitial lung disease in smokers from the COPDGene Study
- PMID: 19781963
- PMCID: PMC2790552
- DOI: 10.1016/j.acra.2009.07.016
Identification of early interstitial lung disease in smokers from the COPDGene Study
Abstract
Rationale and objectives: The aim of this study is to compare two subjective methods for the identification of changes suggestive of early interstitial lung disease (ILD) on chest computed tomographic (CT) scans.
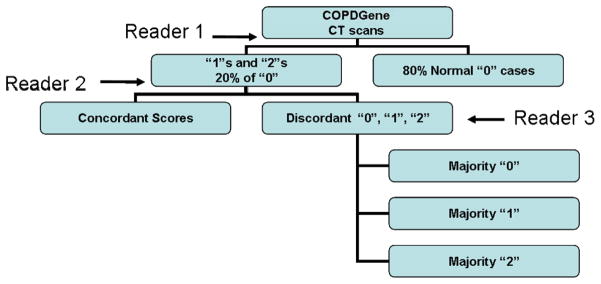
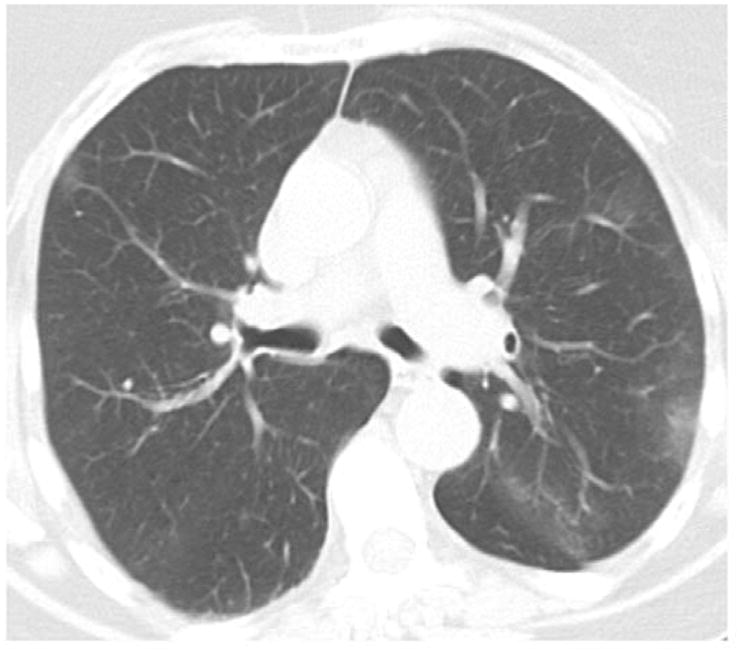
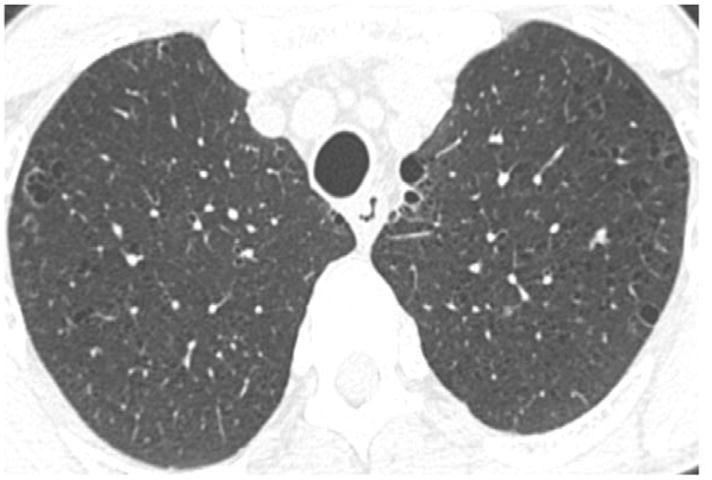
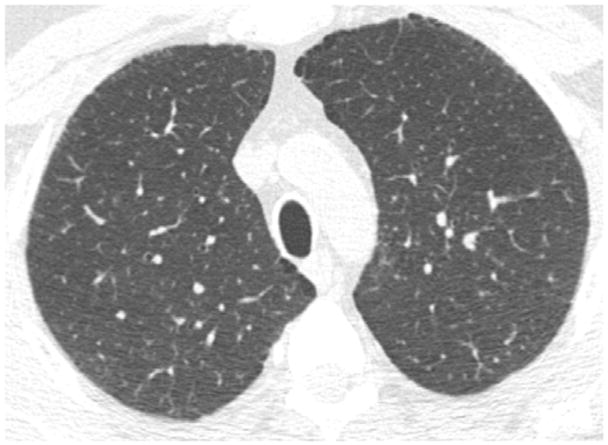
Materials and methods: The CT scans of the first 100 subjects enrolled in the COPDGene Study from a single institution were examined using a sequential reader and a group consensus interpretation scheme. CT scans were evaluated for the presence of parenchymal changes consistent with ILD using the following scoring system: 0 = normal, 1 = equivocal for the presence of ILD, 2 = highly suspicious for ILD, and 3 = classic ILD changes. A statistical comparison of patients with early ILD to normal subjects was performed.
Results: There was a high degree of agreement between methods (kappa = 0.84; 95% confidence interval, 0.73-0.94; P < .0001 for the sequential and consensus methods). The sequential reading method had both high positive (1.0) and negative (0.97) predictive values for a consensus read despite a 58% reduction in the number of chest CT evaluations. Regardless of interpretation method, the prevalence of chest CT changes consistent with early ILD in this subset of smokers from COPDGene varied between 5% and 10%. Subjects with early ILD tended to have greater tobacco smoke exposure than subjects without early ILD (P = .053).
Conclusions: A sequential CT interpretation scheme is an efficient method for the visual interpretation of CT data. Further investigation is required to independently confirm our findings and further characterize early ILD in smokers.
Figures

References
-
- King TEJ, Tooze JA, Schwarz MI, Brown KR, Cherniack RM. Predicting Survival in Idiopathic Pulmonary Fibrosis. Scoring System and Survival Model. Am J Respir Crit Care Med. 2001;164:1171–1181. - PubMed
-
- Raghu G, Weycker D, Edelsberg J, Bradford WZ, Oster G. Incidence and Prevalence of Idiopathic Pulmonary Fibrosis. Am J Respir Crit Care Med. 2006;174:810–816. - PubMed
-
- Gross TJ, Hunninghake GW. Idiopathic Pulmonary Fibrosis. N Engl J Med. 2001;345:517–525. - PubMed
-
- Demedts M, Behr J, Buhl R, et al. High-Dose Acetylcysteine in Idiopathic Pulmonary Fibrosis. N Engl J Med. 2005;353:2229–2242. - PubMed
-
- King TE, Jr, Behr J, Brown KK, et al. BUILD-1: A Randomized Placebo-controlled Trial of Bosentan in Idiopathic Pulmonary Fibrosis. Am J Respir Crit Care Med. 2008;177:75–81. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
