

Noninvasive assessment of left ventricular assist devices with cardiovascular computed tomography and impact on management
- PMID: 19782594
- PMCID: PMC2818038
- DOI: 10.1016/j.healun.2009.06.023
Noninvasive assessment of left ventricular assist devices with cardiovascular computed tomography and impact on management
Abstract
Background: Left ventricular assist devices (LVADs) provide a bridge to recovery or heart transplantation but require serial assessment. Echocardiographic approaches may be limited by device artifact and acoustic window. Cardiovascular computed tomography (CCT) may provide improved non-invasive imaging of LVADs. We evaluated the diagnostic findings and clinical impact of CCT for non-invasive assessment of patients with LVADs.
Methods: CCT examinations performed between 2005 and 2008 in patients with LVADs were identified. Acquisitions were completed on the identical 64-detector-row scanner with intravenous contrast administration. Electrocardiographic gating was used in patients with pulsatile devices, and peripheral pulse gating was used in patients with continuous-flow devices. Comparison was made between CCT results and 30-day outcomes, including echocardiographic and intraoperative findings.
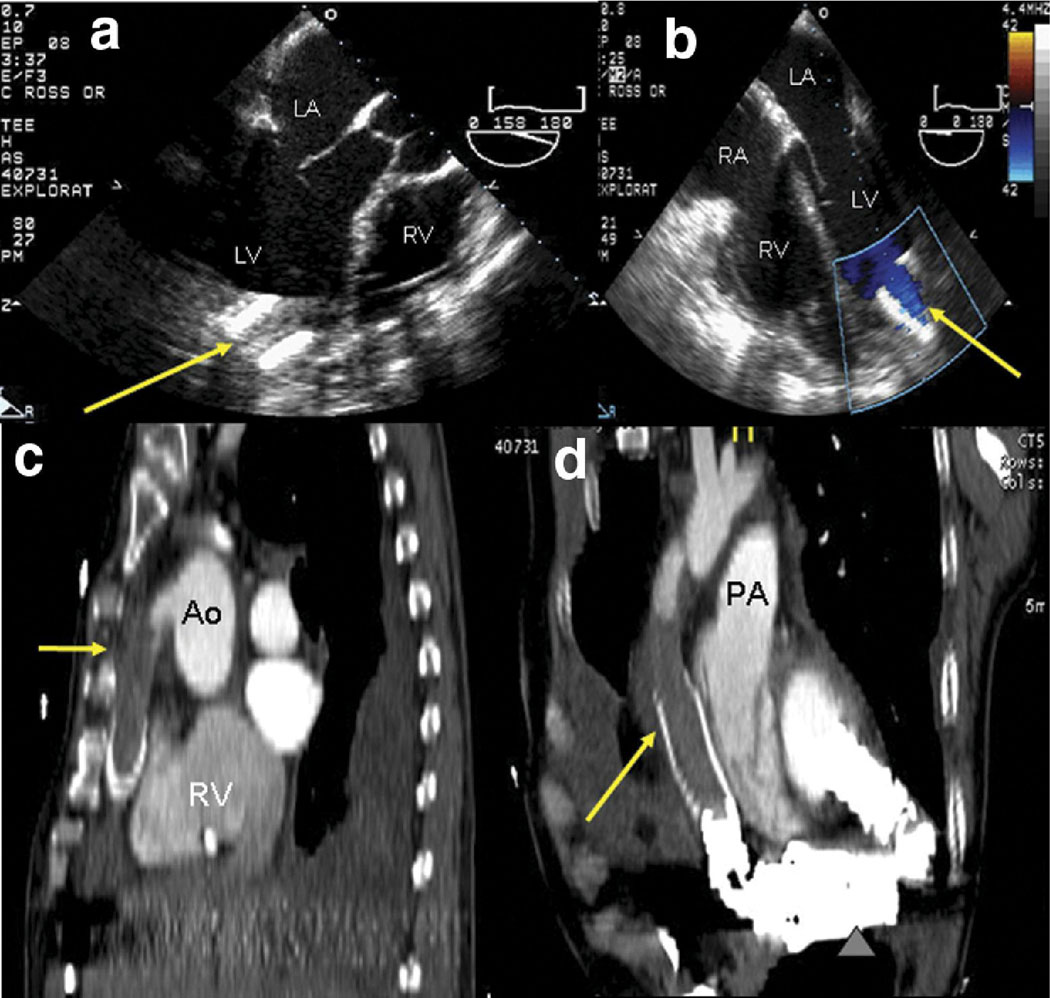
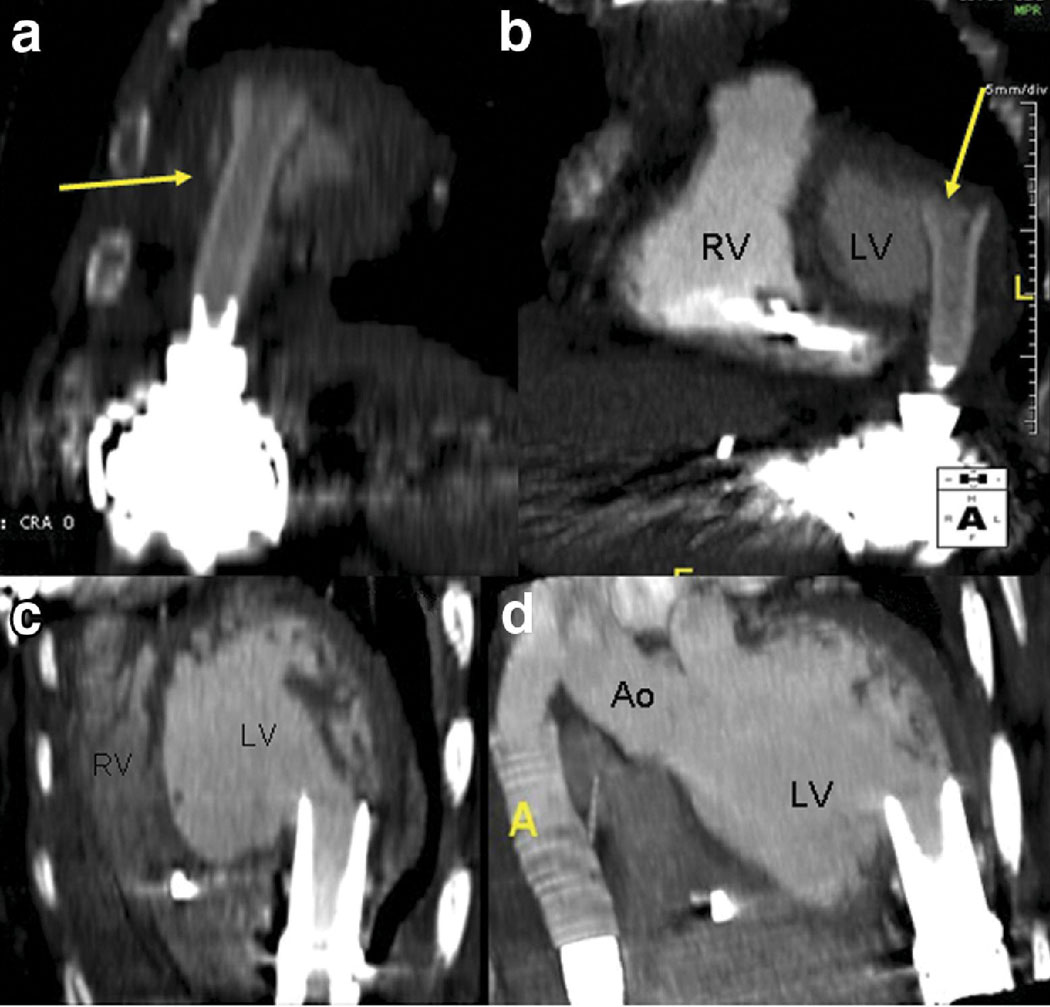
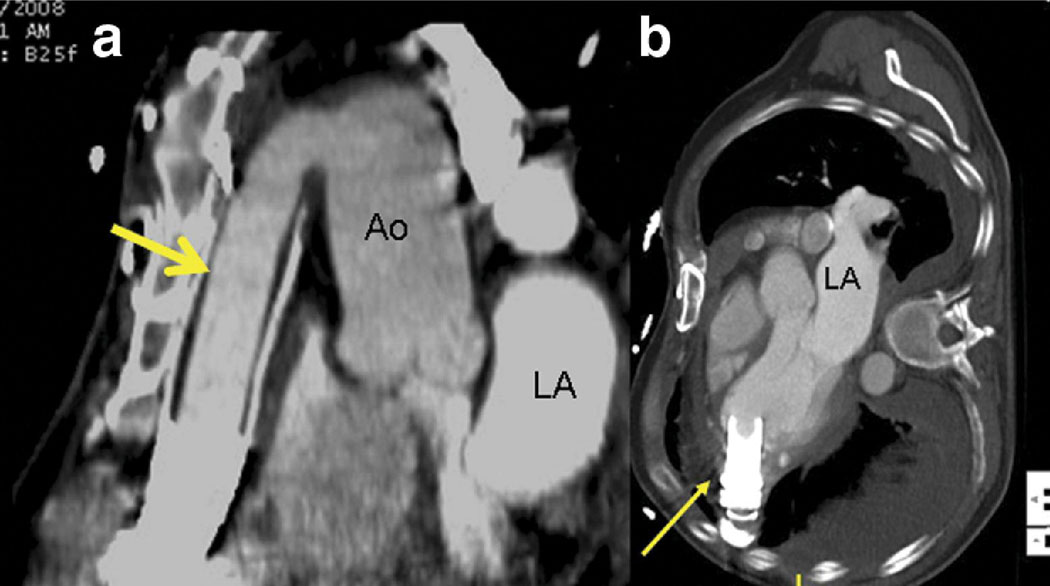
Results: We reviewed 32 CCT examinations from 28 patients. Indications included evaluation of low cardiac output symptoms, assessment of cannula position, low flow reading on the LVAD, and surgical planning. CCT identified critical findings in 6 patients, including thrombosis and inlet cannula malposition, all confirmed intraoperatively. CCT missed 1 case of intra-LVAD thrombus. Using intraoperative findings as the gold standard, CCT's sensitivity was 85% and specificity was 100%. Echocardiographic LVAD evaluation did not correlate with findings on CCT (kappa = -0.29, 95% confidence interval, -0.73 to 0.13).
Conclusions: This preliminary observational cohort study indicates that non-invasive imaging using CCT of LVADs is feasible and accurate. CCT warrants consideration in the initial evaluation of symptomatic patients with LVADs.
Copyright (c) 2010 International Society for Heart and Lung Transplantation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Drs. Sahu, Merchant, Louis IV, Firstenberg, and Sun have no conflicts.
Figures
References
-
- Pennock JL, Pierce WS, Campbell DB, et al. Mechanical support of the circulation followed by cardiac transplantation. J Thorac Cardiovasc Surg. 1986;92:994–1004. - PubMed
-
- Rose EA, Gelijns AC, Moskowitz AJ, et al. Long-term mechanical left ventricular assistance for end-stage heart failure. N Engl J Med. 2001;345:1435–1443. - PubMed
-
- Boyle A. Current status of cardiac transplantation and mechanical circulatory support. Curr Heart Fail Rep. 2009;6:28–33. - PubMed
-
- Piccione W., Jr Left ventricular assist device implantation: short and long-term surgical complications. J Heart Lung Transplant. 2000;19:S89–S94. - PubMed
-
- Catena E, Milazzo F. Echocardiography and cardiac assist devices. Minerva Cardioangiol. 2007;55:247–265. - PubMed
