

Emergency medical services intervals and survival in trauma: assessment of the "golden hour" in a North American prospective cohort
- PMID: 19783323
- PMCID: PMC3008652
- DOI: 10.1016/j.annemergmed.2009.07.024
Emergency medical services intervals and survival in trauma: assessment of the "golden hour" in a North American prospective cohort
Abstract
Study objective: The first hour after the onset of out-of-hospital traumatic injury is referred to as the "golden hour," yet the relationship between time and outcome remains unclear. We evaluate the association between emergency medical services (EMS) intervals and mortality among trauma patients with field-based physiologic abnormality.
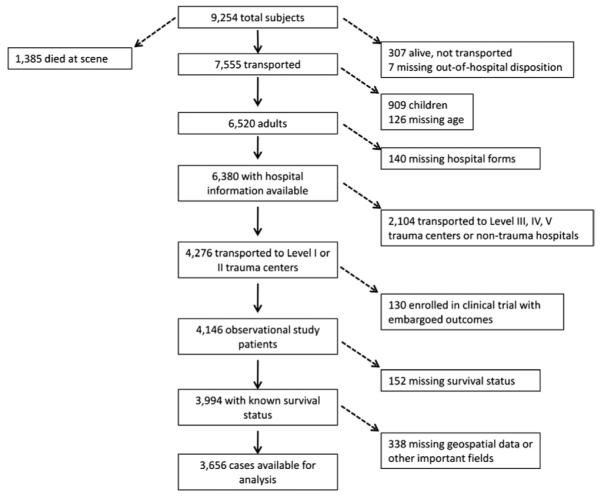
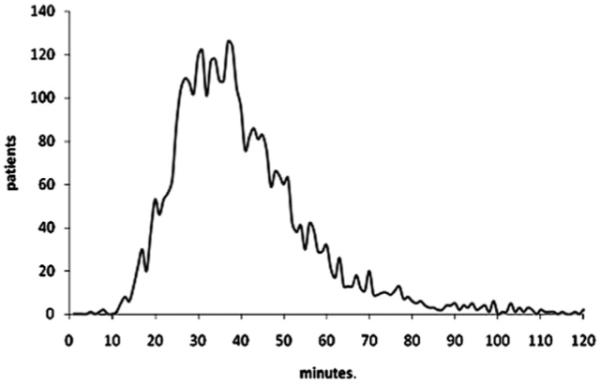
Methods: This was a secondary analysis of an out-of-hospital, prospective cohort registry of adult (aged > or =15 years) trauma patients transported by 146 EMS agencies to 51 Level I and II trauma hospitals in 10 sites across North America from December 1, 2005, through March 31, 2007. Inclusion criteria were systolic blood pressure less than or equal to 90 mm Hg, respiratory rate less than 10 or greater than 29 breaths/min, Glasgow Coma Scale score less than or equal to 12, or advanced airway intervention. The outcome was in-hospital mortality. We evaluated EMS intervals (activation, response, on-scene, transport, and total time) with logistic regression and 2-step instrumental variable models, adjusted for field-based confounders.
Results: There were 3,656 trauma patients available for analysis, of whom 806 (22.0%) died. In multivariable analyses, there was no significant association between time and mortality for any EMS interval: activation (odds ratio [OR] 1.00; 95% confidence interval [CI] 0.95 to 1.05), response (OR 1.00; 95% CI 9.97 to 1.04), on-scene (OR 1.00; 95% CI 0.99 to 1.01), transport (OR 1.00; 95% CI 0.98 to 1.01), or total EMS time (OR 1.00; 95% CI 0.99 to 1.01). Subgroup and instrumental variable analyses did not qualitatively change these findings.
Conclusion: In this North American sample, there was no association between EMS intervals and mortality among injured patients with physiologic abnormality in the field.
Copyright (c) 2009 American College of Emergency Physicians. Published by Mosby, Inc. All rights reserved.
Figures
Comment in
-
Annals of Emergency Medicine Journal Club. Is the golden hour tarnished? Registries and multivariable regression.Ann Emerg Med. 2010 Mar;55(3):247-8. doi: 10.1016/j.annemergmed.2010.01.001. Ann Emerg Med. 2010. PMID: 20171461
-
Annals of emergency medicine journal club. Is the golden hour tarnished? Registries and multivariable regression: answers to the March 2010 journal club questions.Ann Emerg Med. 2010 Aug;56(2):188-200. doi: 10.1016/j.annemergmed.2010.04.003. Ann Emerg Med. 2010. PMID: 20643270 No abstract available.
-
Have we killed the golden hour of trauma?Ann Emerg Med. 2011 Jan;57(1):73-4; author reply 74-5. doi: 10.1016/j.annemergmed.2010.08.003. Ann Emerg Med. 2011. PMID: 21183089 No abstract available.
References
-
- Lerner EB, Moscati RM. The golden hour: scientific fact or medical “urban legend”? Acad Emerg Med. 2001;8:758–760. - PubMed
-
- Sampalis JS, Denis R, Lavoie A, et al. Trauma care regionalization: a process-outcome evaluation. J Trauma. 1999;46:565–581. - PubMed
-
- Samplais JS, Lavoie A, Williams JI, et al. Impact of on-site care, prehospital time, and level of in-hospital care on survival in severely injured patients. J Trauma. 1993;34:252–261. - PubMed
-
- Pepe PE, Wyatt CH, Bickell WH, et al. The relationship between total prehospital time and outcome in hypotensive victims of penetrating injuries. Ann Emerg Med. 1987;16:293–297. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 HL077866/HL/NHLBI NIH HHS/United States
- U01 HL077871/HL/NHLBI NIH HHS/United States
- CAPMC/ CIHR/Canada
- HL077867/HL/NHLBI NIH HHS/United States
- 5U01 HL077863/HL/NHLBI NIH HHS/United States
- U01 HL077881/HL/NHLBI NIH HHS/United States
- HL077873/HL/NHLBI NIH HHS/United States
- U01 HL077872/HL/NHLBI NIH HHS/United States
- HL077871/HL/NHLBI NIH HHS/United States
- HL077881/HL/NHLBI NIH HHS/United States
- HL077908/HL/NHLBI NIH HHS/United States
- HL077877/HL/NHLBI NIH HHS/United States
- U01 HL077885/HL/NHLBI NIH HHS/United States
- U01 HL077863/HL/NHLBI NIH HHS/United States
- U01 HL077908/HL/NHLBI NIH HHS/United States
- HL077872/HL/NHLBI NIH HHS/United States
- HL077866/HL/NHLBI NIH HHS/United States
- U01 HL077873/HL/NHLBI NIH HHS/United States
- U01 HL077867/HL/NHLBI NIH HHS/United States
- HL077885/HL/NHLBI NIH HHS/United States
