

The impact of fluoride on ameloblasts and the mechanisms of enamel fluorosis
- PMID: 19783795
- PMCID: PMC3318083
- DOI: 10.1177/0022034509343280
The impact of fluoride on ameloblasts and the mechanisms of enamel fluorosis
Abstract
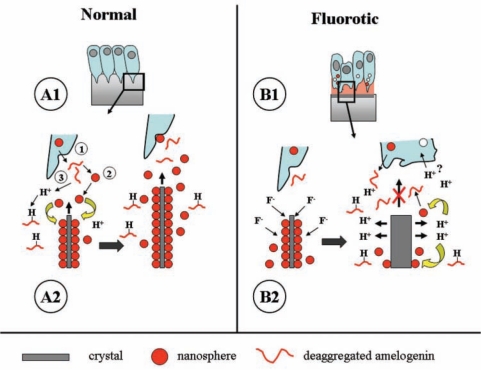
Intake of excess amounts of fluoride during tooth development cause enamel fluorosis, a developmental disturbance that makes enamel more porous. In mild fluorosis, there are white opaque striations across the enamel surface, whereas in more severe cases, the porous regions increase in size, with enamel pitting, and secondary discoloration of the enamel surface. The effects of fluoride on enamel formation suggest that fluoride affects the enamel-forming cells, the ameloblasts. Studies investigating the effects of fluoride on ameloblasts and the mechanisms of fluorosis are based on in vitro cultures as well as animal models. The use of these model systems requires a biologically relevant fluoride dose, and must be carefully interpreted in relation to human tooth formation. Based on these studies, we propose that fluoride can directly affect the ameloblasts, particularly at high fluoride levels, while at lower fluoride levels, the ameloblasts may respond to local effects of fluoride on the mineralizing matrix. A new working model is presented, focused on the assumption that fluoride increases the rate of mineral formation, resulting in a greater release of protons into the forming enamel matrix.
Figures
References
-
- Andersen L, Richards A, Care AD, Andersen HM, Kragstrup J, Fejerskov O. (1986). Parathyroid glands, calcium, and vitamin D in experimental fluorosis in pigs. Calcif Tissue Int 38:222-226 - PubMed
-
- Angmar-Månsson B, Whitford GM. (1982). Plasma fluoride levels and enamel fluorosis in the rat. Caries Res 16:334-339 - PubMed
-
- Angmar-Månsson B, Whitford GM. (1984). Enamel fluorosis related to plasma F levels in the rat. Caries Res 18:25-32 - PubMed
-
- Angmar-Månsson B, Whitford GM. (1985). Single fluoride doses and enamel fluorosis in the rat. Caries Res 19:145-152 - PubMed
-
- Angmar-Månsson B, Ericsson Y, Ekberg O. (1976). Plasma fluoride and enamel fluorosis. Calcif Tissue Res 22:77-84 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
