

Discovery and identification of potential biomarkers of papillary thyroid carcinoma
- PMID: 19785722
- PMCID: PMC2761863
- DOI: 10.1186/1476-4598-8-79
Discovery and identification of potential biomarkers of papillary thyroid carcinoma
Abstract
Background: Thyroid carcinoma is the most common endocrine malignancy and a common cancer among the malignancies of head and neck. Noninvasive and convenient biomarkers for diagnosis of papillary thyroid carcinoma (PTC) as early as possible remain an urgent need. The aim of this study was to discover and identify potential protein biomarkers for PTC specifically.
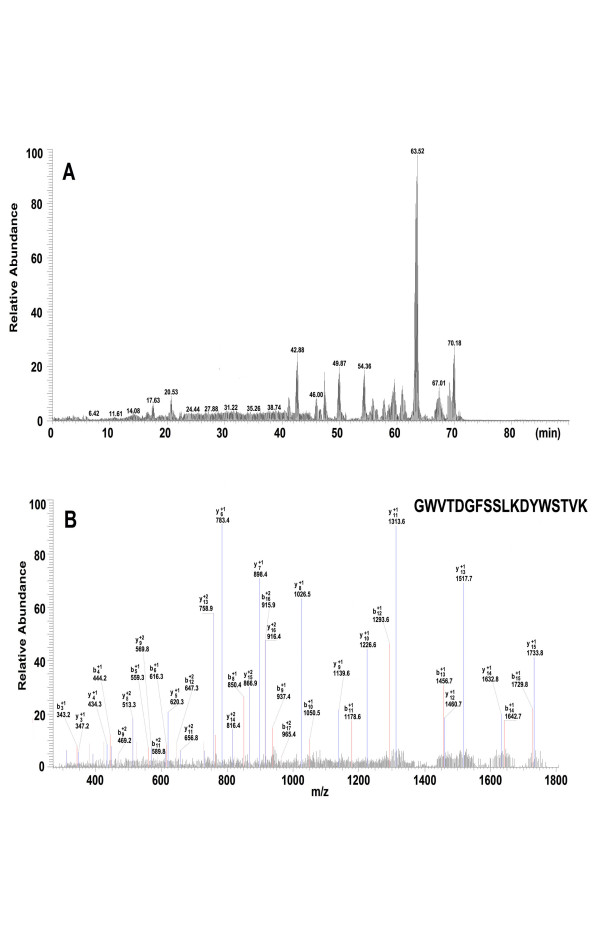
Methods: Two hundred and twenty four (224) serum samples with 108 PTC and 116 controls were randomly divided into a training set and a blind testing set. Serum proteomic profiles were analyzed using SELDI-TOF-MS. Candidate biomarkers were purified by HPLC, identified by LC-MS/MS and validated using ProteinChip immunoassays.
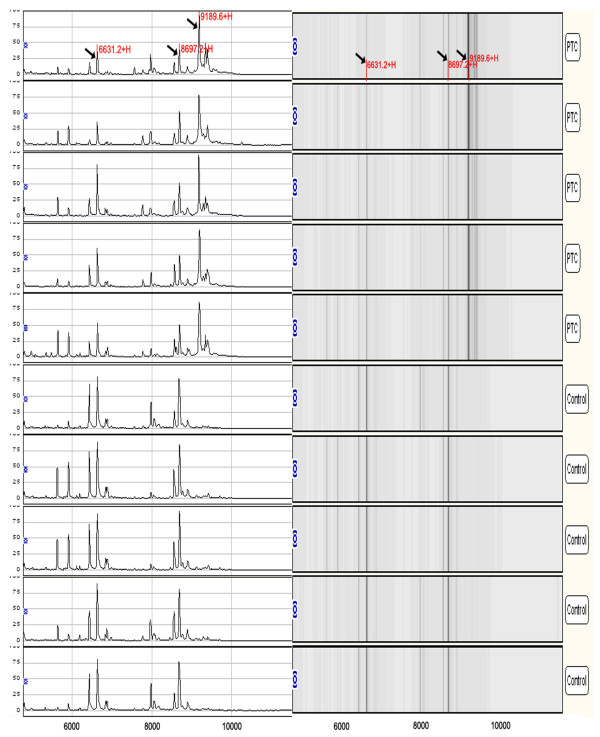
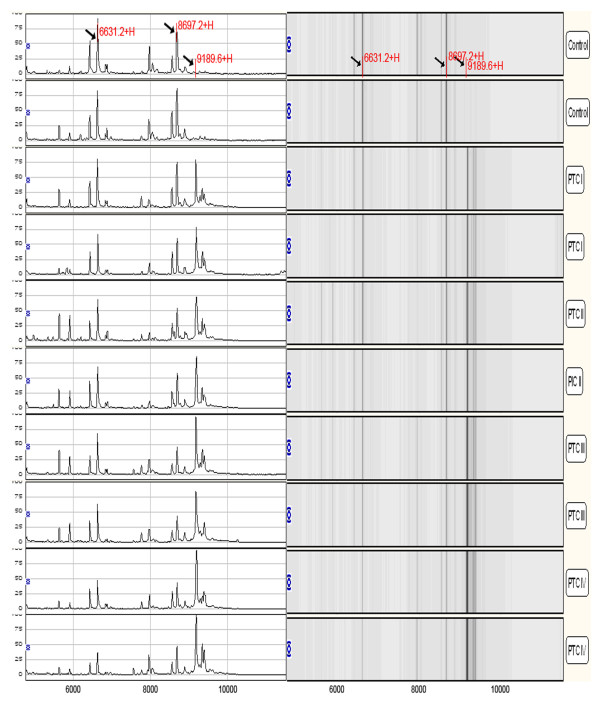
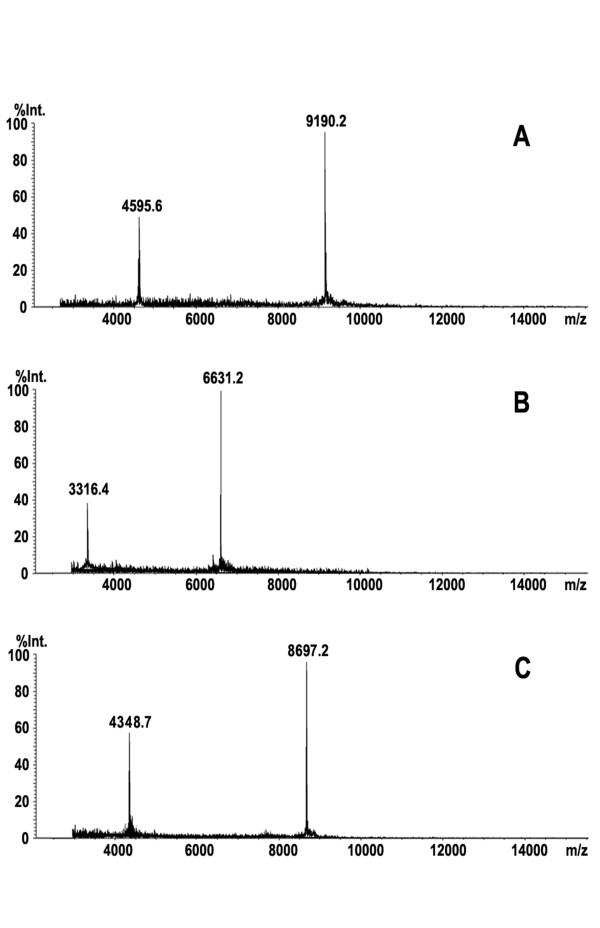
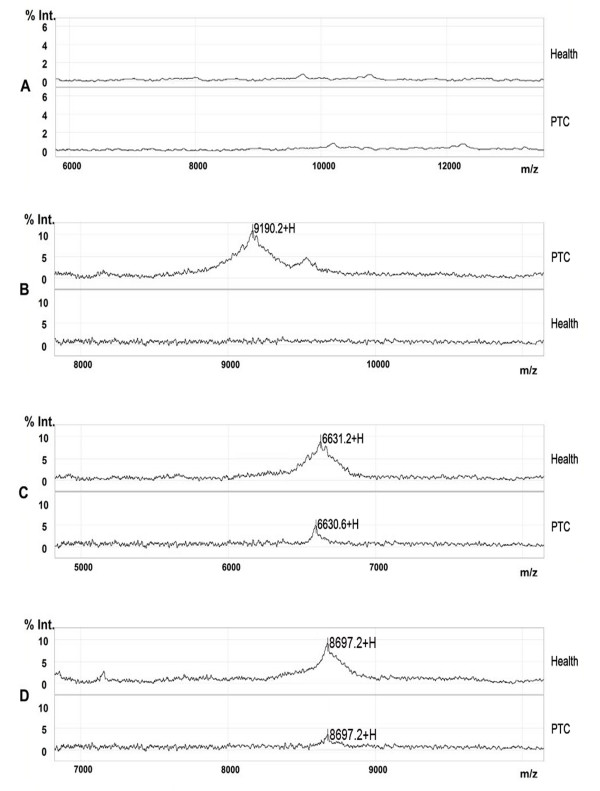
Results: A total of 3 peaks (m/z with 9190, 6631 and 8697 Da) were screened out by support vector machine (SVM) to construct the classification model with high discriminatory power in the training set. The sensitivity and specificity of the model were 95.15% and 93.97% respectively in the blind testing set. The candidate biomarker with m/z of 9190 Da was found to be up-regulated in PTC patients, and was identified as haptoglobin alpha-1 chain. Another two candidate biomarkers (6631, 8697 Da) were found down-regulated in PTC and identified as apolipoprotein C-I and apolipoprotein C-III, respectively. In addition, the level of haptoglobin alpha-1 chain (9190 Da) progressively increased with the clinical stage I, II, III and IV, and the expression of apolipoprotein C-I and apolipoprotein C-III (6631, 8697 Da) gradually decreased in higher stages.
Conclusion: We have identified a set of biomarkers that could discriminate PTC from non-cancer controls. An efficient strategy, including SELDI-TOF-MS analysis, HPLC purification, MALDI-TOF-MS trace and LC-MS/MS identification, has been proved successful.
Figures
References
-
- Pelizzo MR, Merante Boschin I, Toniato A, Casal Ide E, Mian C, Rubello D, Pagetta C. Diagnosis, treatment, prognostic factors and long-term outcome in papillary thyroid carcinoma. Minerva Endocrinol. 2008;33:359–379. - PubMed
-
- Hayashi N, Kitaoka M. Fine-needle aspiration biopsy of the thyroid nodule: uses and limitations. Nippon Rinsho. 2007;65:2003–2007. - PubMed
-
- Inohara H, Segawa T, Miyauchi A, Yoshii T, Nakahara S, Raz A, Maeda M, Miyoshi E, Kinoshita N, Yoshida H, Furukawa M, Takenaka Y, Takamura Y, Ito Y, Taniguchi N. Cytoplasmic and serum galectin-3 in diagnosis of thyroid malignancies. Biochem Biophys Res Commun. 2008;376:605–610. doi: 10.1016/j.bbrc.2008.09.041. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
