

Initial experience of laparostomy with immediate vacuum therapy in patients with severe peritonitis
- PMID: 19785944
- PMCID: PMC2966252
- DOI: 10.1308/003588409X12486167520993
Initial experience of laparostomy with immediate vacuum therapy in patients with severe peritonitis
Abstract
Introduction: To report our initial experience of laparostomy and immediate intra-abdominal vacuum therapy in patients with severe peritonitis due to intra-abdominal catastrophes.
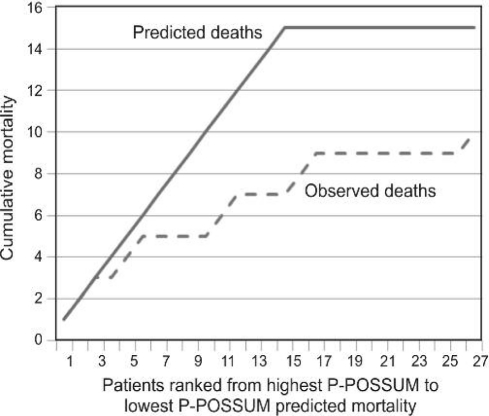
Patients and methods: Twenty-seven patients underwent emergency laparotomy and laparostomy formation with the application of immediate intra-abdominal TRAC-VAC therapy (male:female ratio, 1:1.2; median age, 73 years; range, 34-84 years). Predicted mortality was assessed using the P-POSSUM score and compared with clinically observed outcomes.
Results: Ten patients (37%) with a mean predicted P-POSSUM mortality of 72%, died of sepsis and multi-organ failure. Seventeen patients (mean P-POSSUM 48% expected mortality) survived to discharge. One patient with pancreatitis died from small bowel obstruction 1-year post discharge, two patients developed a small bowel fistula. One patient had an allergic reaction to the VAC dressing. Our patients, treated with laparostomy and TRAC VAC therapy, had a significantly improved observed survival when compared to P-POSSUM expected survival (P = 0.004).
Conclusions: Laparostomy with immediate intraperitoneal VAC therapy is a robust and effective system to manage patients with intra-abdominal catastrophes. There were significantly improved outcomes compared to the mortality predicted by P-POSSUM scores. Damage control surgery with laparostomy formation and intra-abdominal VAC therapy should be considered in patients with severe peritonitis.
Figures
References
-
- Hadeed JG, Staman GW, Sariol HS, Kumar S, Ross SE. Delayed primary closure in damage control laparotomy: the value of the Wittmann patch. Am Surg. 2007;73:10–2. - PubMed
-
- Chorbadjian M, Bown M, Graham C, Sayers R. Laparostomy healing by secondary intention after ruptured abdominal aortic aneurysm repair. J Tissue Viability. 2004;14:24–7. - PubMed
-
- Finlay IG, Edwards TJ, Lambert AW. Damage control laparotomy. Br J Surg. 2004;91:83–5. - PubMed
-
- de Laet IE, Malbrain M. Current insights in intra-abdominal hypertension and abdominal compartment syndrome. Med Intensiva. 2007;31:88–99. - PubMed
-
- Brox-Jimenez A, Ruiz-luque V, Torres-Arros C. Experience with the Bogata bag technique for temporary abdominal closure. Cir Esp. 2007;83:150–4. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources