

Predictors of technical success and postnatal biventricular outcome after in utero aortic valvuloplasty for aortic stenosis with evolving hypoplastic left heart syndrome
- PMID: 19786635
- PMCID: PMC4235336
- DOI: 10.1161/CIRCULATIONAHA.109.848994
Predictors of technical success and postnatal biventricular outcome after in utero aortic valvuloplasty for aortic stenosis with evolving hypoplastic left heart syndrome
Abstract
Background: Aortic stenosis in the midgestation fetus with a normal-sized or dilated left ventricle predictably progresses to hypoplastic left heart syndrome when associated with certain physiological findings. Prenatal balloon aortic valvuloplasty may improve left heart growth and function, possibly preventing evolution to hypoplastic left heart syndrome.
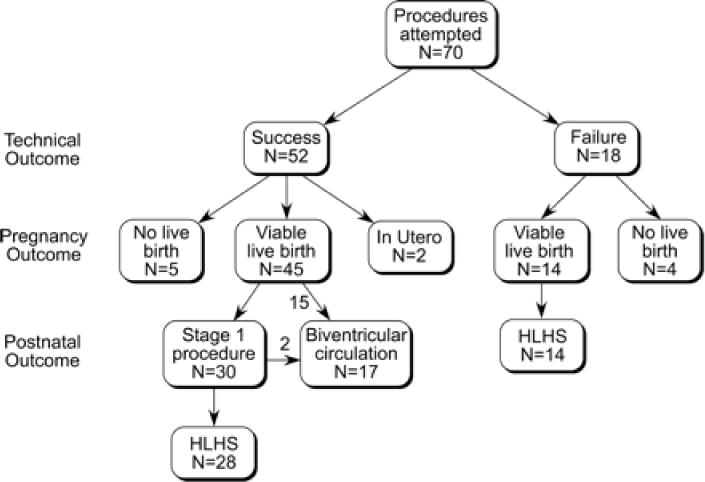
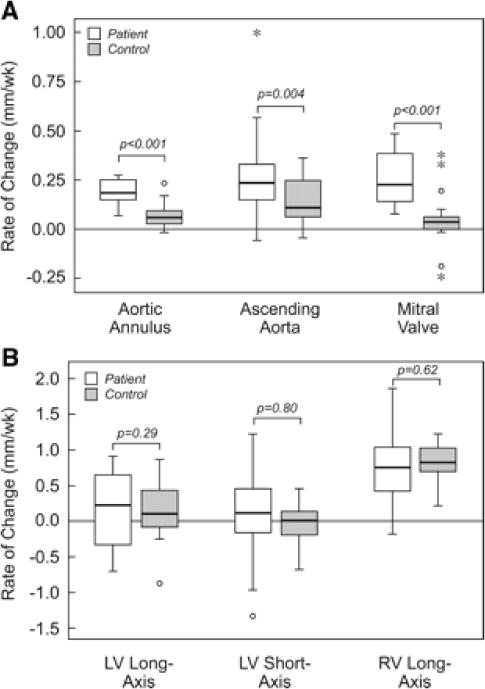
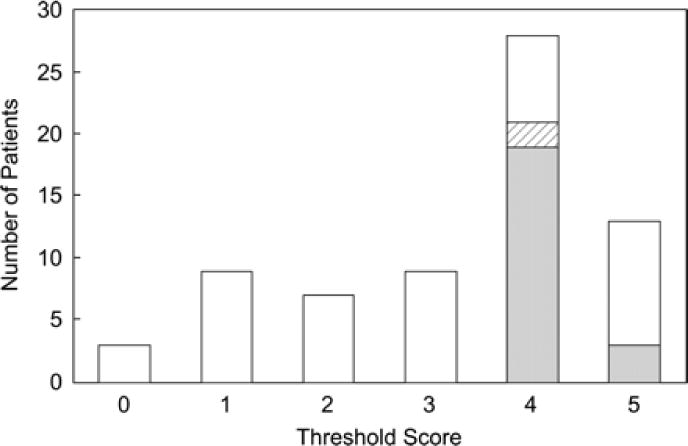
Methods and results: Between March 2000 and October 2008, 70 fetuses underwent attempted aortic valvuloplasty for critical aortic stenosis with evolving hypoplastic left heart syndrome. We analyzed this experience to determine factors associated with procedural and postnatal outcome. The median gestational age at intervention was 23 weeks. The procedure was technically successful in 52 fetuses (74%). Relative to 21 untreated comparison fetuses, subsequent prenatal growth of the aortic and mitral valves, but not the left ventricle, was improved after intervention. Nine pregnancies (13%) did not reach a viable term or preterm birth. Seventeen patients had a biventricular circulation postnatally, 15 from birth. Larger left heart structures and higher left ventricular pressure at the time of intervention were associated with biventricular outcome. A multivariable threshold scoring system was able to discriminate fetuses with a biventricular outcome with 100% sensitivity and modest positive predictive value.
Conclusions: Technically successful aortic valvuloplasty alters left heart valvar growth in fetuses with aortic stenosis and evolving hypoplastic left heart syndrome and, in a subset of cases, appeared to contribute to a biventricular outcome after birth. Fetal aortic valvuloplasty carries a risk of fetal demise. Fetuses undergoing in utero aortic valvuloplasty with an unfavorable multivariable threshold score at the time of intervention are very unlikely to achieve a biventricular circulation postnatally.
Figures

References
-
- Mahle WT, Spray TL, Wernovsky G, Gaynor JW, Clark BJ. Survival after reconstructive surgery for hypoplastic left heart syndrome: a 15-year experience from a single institution. Circulation. 2000;102(suppl):III-136–III-141. - PubMed
-
- Tweddell JS, Hoffman GM, Mussatto KA, Fedderly RT, Berger S, Jaquiss RD, Ghanayem NS, Frisbee SJ, Litwin SB. Improved survival of patients undergoing palliation of hypoplastic left heart syndrome: lessons learned from 115 consecutive patients. Circulation. 2002;106(suppl):I-82–II-89. - PubMed
-
- Tabbutt S, Dominguez TE, Ravishankar C, Marino BS, Gruber PJ, Wernovsky G, Gaynor JW, Nicolson SC, Spray TL. Outcomes after the stage I reconstruction comparing the right ventricular to pulmonary artery conduit with the modified Blalock Taussig shunt. Ann Thorac Surg. 2005;80:1582–1590. - PubMed
-
- Danford DA, Cronican P. Hypoplastic left heart syndrome: progression of left ventricular dilation and dysfunction to left ventricular hypoplasia in utero. Am Heart J. 1992;123:1712–1713. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
