

The impact of ischemic cholangiopathy in liver transplantation using donors after cardiac death: the untold story
- PMID: 19789011
- PMCID: PMC2790600
- DOI: 10.1016/j.surg.2009.06.052
The impact of ischemic cholangiopathy in liver transplantation using donors after cardiac death: the untold story
Abstract
Background: Liver transplantation (LT) from donation after cardiac death (DCD) donors is increasingly being used to address organ shortages. Despite encouraging reports, standard survival metrics have overestimated the effectiveness of DCD livers. We examined the mode, kinetics, and predictors of organ failure and resource utilization to more fully characterize outcomes after DCD LT.
Methods: We reviewed the outcomes for 32 DCD and 237 donation after brain death (DBD) LT recipients at our institution.
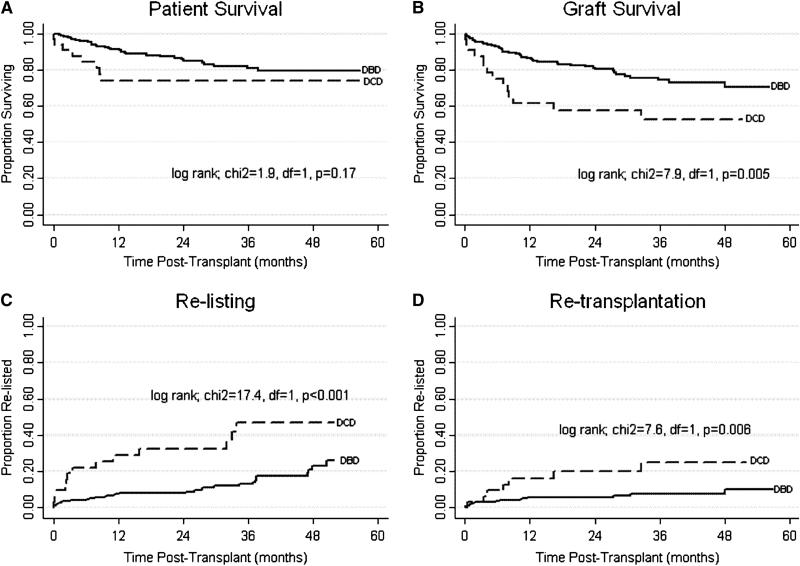
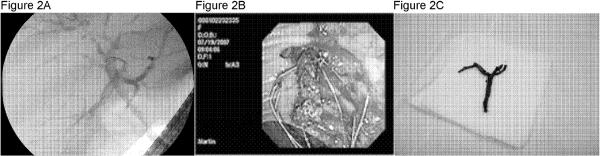
Results: Recipients of DCD livers had a 2.1 times greater risk of graft failure, a 2.5 times greater risk of relisting, and a 3.2 times greater risk of retransplantation compared with DBD recipients. DCD recipients had a 31.6% higher incidence of biliary complications and a 35.8% higher incidence of ischemic cholangiopathy. Ischemic cholangiography was primarily implicated in the higher risk of graft failure observed after DCD LT. DCD recipients with ischemic cholangiography experienced more frequent rehospitalizations, longer hospital stays, and required more invasive biliary procedures.
Conclusion: Related to higher complication rates, DCD recipients necessitated greater resource utilization. This more granular data should be considered in the decision to promote DCD LT. Modification of liver allocation policy is necessary to address those disadvantaged by a failing DCD graft.
Figures
References
-
- Pomfret EA. Solving the organ shortage crisis: the 7th annual American Society of Transplant Surgeons' State-of-the-Art Winter Symposium. Am J Transplant. 2008;8(4):745–52. - PubMed
-
- Freeman RB, Jr., et al. Liver and intestine transplantation in the United States, 1997–2006. Am J Transplant. 2008;8(4 Pt 2):958–76. - PubMed
-
- Medicare and Medicaid programs; conditions for coverage for organ procurement organizations (OPOs). Final rule. Fed Regist. 2006;71(104):30981–1054. - PubMed
-
- Whiting JF, et al. Clinical results of an organ procurement organization effort to increase utilization of donors after cardiac death. Transplantation. 2006;81(10):1368–71. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
