

Thyroid hormone replacement after thyroid lobectomy
- PMID: 19789012
- PMCID: PMC2755641
- DOI: 10.1016/j.surg.2009.06.026
Thyroid hormone replacement after thyroid lobectomy
Abstract
Background: The purpose of this study was to determine the incidence of and identify risk factors for postoperative hypothyroidism in patients undergoing thyroid lobectomy.
Methods: We retrospectively reviewed patients who underwent a thyroid lobectomy for benign disease from May 2004 to December 2007. Patients with known hypothyroidism or on preoperative thyroid hormone replacement were excluded.
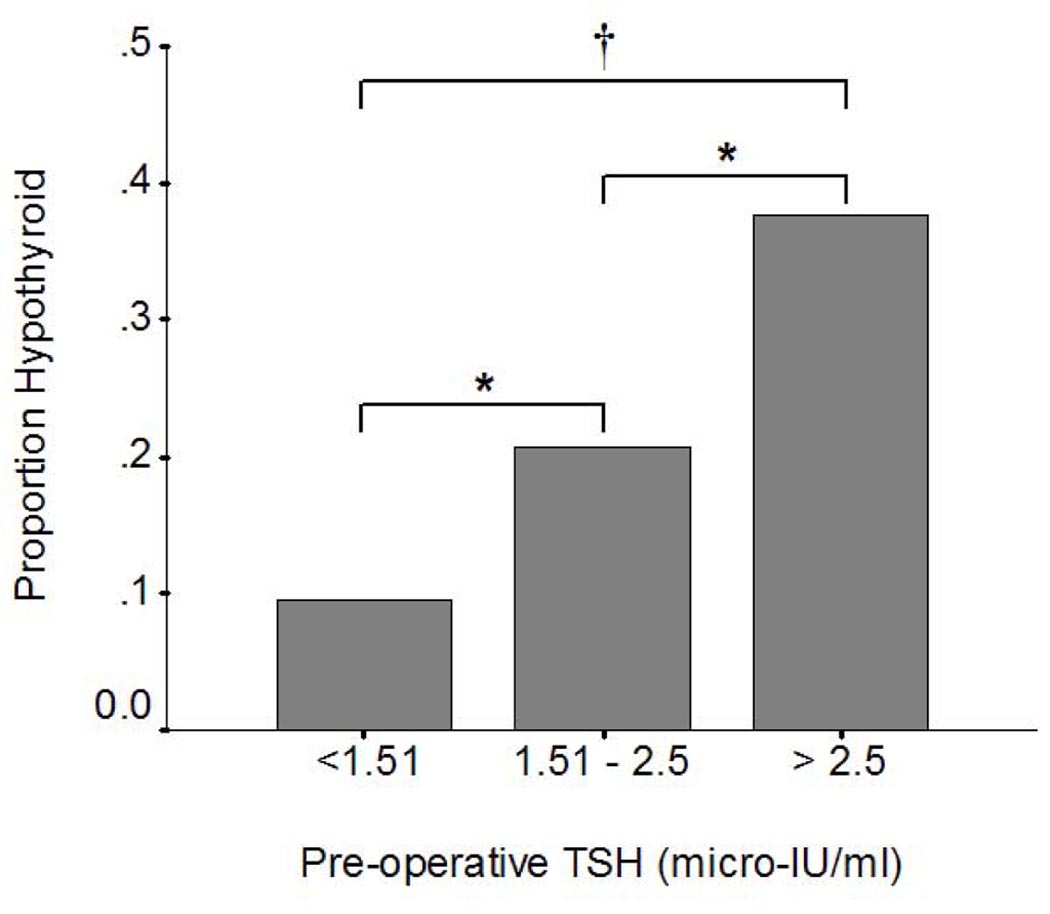
Results: In this study, 14.3% of patients developed hypothyroidism and required thyroid hormone supplementation. These hypothyroid patients had a higher mean pre-operative thyroid-stimulating hormone (TSH) and lower mean free thyroxine (T4) serum levels compared with euthyroid patients (TSH, 2.12 vs 1.35 microIU/mL [P = .006]; free T4, 1.03 vs 1.34 ng/dL [P = .01]). When stratified into 3 groups based on their preoperative TSH measurement (< or =1.5, 1.51-2.5, and > or =2.51 microIU/mL), the rate of hypothyroidism increased significantly at each level (13.5%, 20.5%, and 41.3%, respectively [P < .001]). In addition, patients with Hashimoto's thyroiditis were significantly more likely to become hypothyroid (odds ratio, 3.78; 95% confidence interval, 2.17-6.60).
Conclusion: After thyroid lobectomy, approximately 1 in 7 patients experience hypothyroidism requiring thyroid hormone treatment. Patients with preoperative TSH levels >1.5 microIU/mL, lower free T4 levels, and Hashimoto's thyroiditis are at increased risk and should be counseled and followed appropriately.
Figures
References
-
- Mittendorf E, McHenry C. Thyroidectomy for selected patients with thyrotoxicosis. Arch Otolaryngol Head Neck Surg. 2001 Jan;127(1):61–65. - PubMed
-
- Fewins J, Simpson C, Miller F. Complications of thyroid and parathyroid surgery. Otolaryngol Clin North Am. 2003 Feb;36(1):189–206. x. - PubMed
-
- Bergfelt G, Risholm L. Postoperative thyroid hormone therapy in nontoxic goitre. Acta Chir Scand. 1963 Dec;126:531–537. - PubMed
-
- Berglund J, Bondesson L, Christensen S, Larsson A, Tibblin S. Indications for thyroxine therapy after surgery for nontoxic benign goitre. Acta Chir Scand. 156(6–7):433–438. - PubMed
-
- Hedman I, Jansson S, Lindberg S. Need for thyroxine in patients lobectomised for benign thyroid disease as assessed by follow-up on average fifteen years after surgery. Acta Chir Scand. 152:481–486. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
