

Antiglioma immunological memory in response to conditional cytotoxic/immune-stimulatory gene therapy: humoral and cellular immunity lead to tumor regression
- PMID: 19789315
- PMCID: PMC2796687
- DOI: 10.1158/1078-0432.CCR-09-1087
Antiglioma immunological memory in response to conditional cytotoxic/immune-stimulatory gene therapy: humoral and cellular immunity lead to tumor regression
Abstract
Purpose: Glioblastoma multiforme is a deadly primary brain cancer. Because the tumor kills due to recurrences, we tested the hypothesis that a new treatment would lead to immunological memory in a rat model of recurrent glioblastoma multiforme.
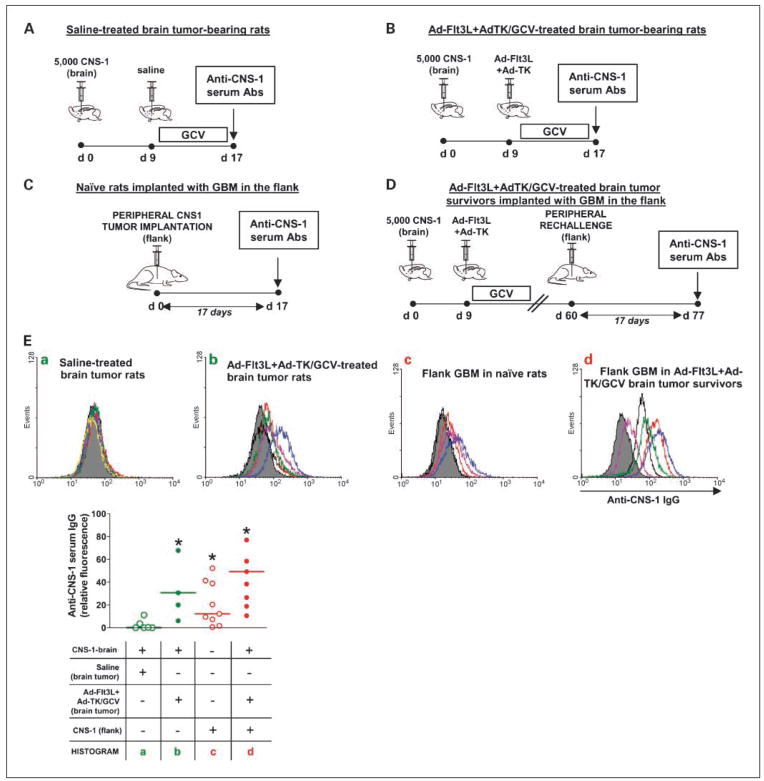
Experimental design: We developed a combined treatment using an adenovirus (Ad) expressing fms-like tyrosine kinase-3 ligand (Flt3L), which induces the infiltration of immune cells into the tumor microenvironment, and an Ad expressing herpes simplex virus-1-thymidine kinase (TK), which kills proliferating tumor cells in the presence of ganciclovir.
Results: This treatment induced immunological memory that led to rejection of a second glioblastoma multiforme implanted in the contralateral hemisphere and of an extracranial glioblastoma multiforme implanted intradermally. Rechallenged long-term survivors exhibited anti-glioblastoma multiforme-specific T cells and displayed specific delayed-type hypersensitivity. Using depleting antibodies, we showed that rejection of the second tumor was dependent on CD8(+) T cells. Circulating anti-glioma antibodies were observed when glioblastoma multiforme cells were implanted intradermally in naïve rats or in long-term survivors. However, rats bearing intracranial glioblastoma multiforme only exhibited circulating antitumoral antibodies upon treatment with Ad-Flt3L + Ad-TK. This combined treatment induced tumor regression and release of the chromatin-binding protein high mobility group box 1 in two further intracranial glioblastoma multiforme models, that is, Fisher rats bearing intracranial 9L and F98 glioblastoma multiforme cells.
Conclusions: Treatment with Ad-Flt3L + Ad-TK triggered systemic anti-glioblastoma multiforme cellular and humoral immune responses, and anti-glioblastoma multiforme immunological memory. Release of the chromatin-binding protein high mobility group box 1 could be used as a noninvasive biomarker of therapeutic efficacy for glioblastoma multiforme. The robust treatment efficacy lends further support to its implementation in a phase I clinical trial.
Conflict of interest statement
No potential conflicts of interest were disclosed.
Figures




References
-
- Chinot OL, Barrie M, Fuentes S, et al. Correlation between O6-methylguanine-DNA methyl-transferase and survival in inoperable newly diagnosed glioblastoma patients treated with neoadjuvant temozolomide. J Clin Oncol. 2007;25:1470–5. - PubMed
-
- Hegi ME, Diserens AC, Gorlia T, et al. MGMT gene silencing and benefit from temozolomide in glioblastoma. N Engl J Med. 2005;352:997–1003. - PubMed
-
- Izquierdo M, Martin V, de Felipe P, et al. Human malignant brain tumor response to herpes simplex thymidine kinase (HSVtk)/ganciclovir gene therapy. Gene Ther. 1996;3:491–5. - PubMed
-
- Klatzmann D, Valery CA, Bensimon G, et al. A phase I/II study of herpes simplex virus type 1 thymidine kinase “suicide” gene therapy for recurrent glioblastoma. Study Group on Gene Therapy for Glioblastoma. Hum Gene Ther. 1998;9:2595–604. - PubMed
-
- Rainov NG. A phase III clinical evaluation of herpes simplex virus type 1 thymidine kinase and ganciclovir gene therapy as an adjuvant to surgical resection and radiation in adults with previously untreated glioblastoma multiforme. Hum Gene Ther. 2000;11:2389–401. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 NS054193/NS/NINDS NIH HHS/United States
- 1R21-NS054143/NS/NINDS NIH HHS/United States
- U01 NS052465/NS/NINDS NIH HHS/United States
- R01 NS061107/NS/NINDS NIH HHS/United States
- 1UO1 NS052465/NS/NINDS NIH HHS/United States
- F32 NS058156/NS/NINDS NIH HHS/United States
- R01 NS042893/NS/NINDS NIH HHS/United States
- 1 RO1 NS 054193/NS/NINDS NIH HHS/United States
- R01 NS057711/NS/NINDS NIH HHS/United States
- R21 NS054143/NS/NINDS NIH HHS/United States
- 1R01-NS057711/NS/NINDS NIH HHS/United States
- 1F32NS050303/NS/NINDS NIH HHS/United States
- R21 NS047298/NS/NINDS NIH HHS/United States
- 1R21 NS047298/NS/NINDS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
