

Imaging metastatic bone disease from carcinoma of the prostate
- PMID: 19789531
- PMCID: PMC2768452
- DOI: 10.1038/sj.bjc.6605334
Imaging metastatic bone disease from carcinoma of the prostate
Abstract
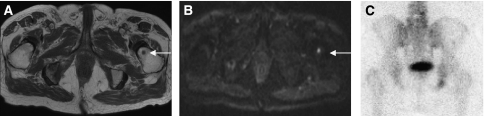
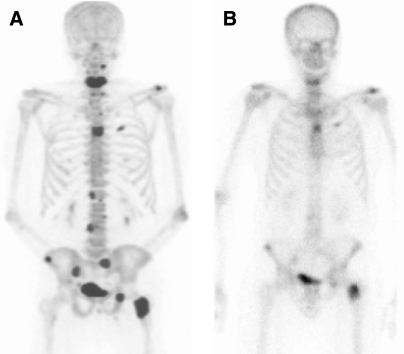
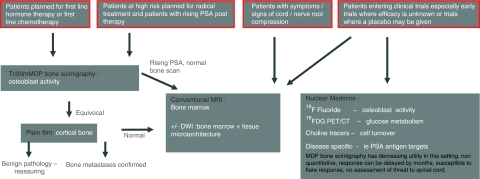
Imaging bone metastases from prostate cancer presents several challenges. The lesions are usually sclerotic and appear late on the conventional X-ray. Bone scintigraphy is the mainstay of lesion detection, but is often not suitable for assessment of treatment response, particularly because of a 'flare' phenomenon after therapy. Magnetic resonance imaging is increasingly used in assessment, and newer techniques allow quantitation. In addition to (18)F-fluorodeoxyglucose ((18)FDG), newer PET isotopes are also showing promise in lesion detection and response assessment. This article reviews the available imaging modalities for evaluating prostatic bony metastases, and links them to the underlying pathological changes within bone lesions.
Figures
References
-
- Algra PR, Bloem J, Tissing H, Falke TH, Arndt JW, Verboom LJ (1991) Detection of vertebral metastases: comparison between MR imaging and bone scintigraphy. Radiographics 11: 219–232 - PubMed
-
- Beheshti M, Vali R, Waldenberger P, Fitz F, Nader M, Loidl W, Broinger G, Stoiber F, Foglman I, Langsteger W (2008) Detection of bone metastases in patients with prostate cancer by 18F fluorocholine and 18 F fluoride PET-CT: a comparative study. Eur J Nucl Med Mol Imaging 35: 1766–1774 - PubMed
-
- Bubendorf L, Schopfer A, Wagner U, Sauter G, Moch H, Wili N, Gasser TC, Mihatsch MJ (2000) Metastatic patterns of prostate cancer: an autopsy study of 1589 patients. Hum Path 31: 578–583 - PubMed
-
- Carlin BI, Andriole GL (2000) The natural history, skeletal complications and management of bone metastases in patients with prostate carcinoma. Cancer 88: 2989–2994 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
