

Diffusion-weighted imaging in head and neck cancers
- PMID: 19792966
- PMCID: PMC2791671
- DOI: 10.2217/fon.09.77
Diffusion-weighted imaging in head and neck cancers
Abstract
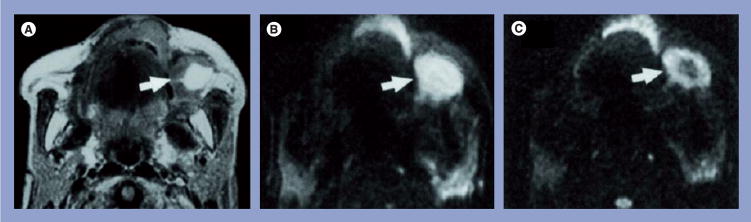
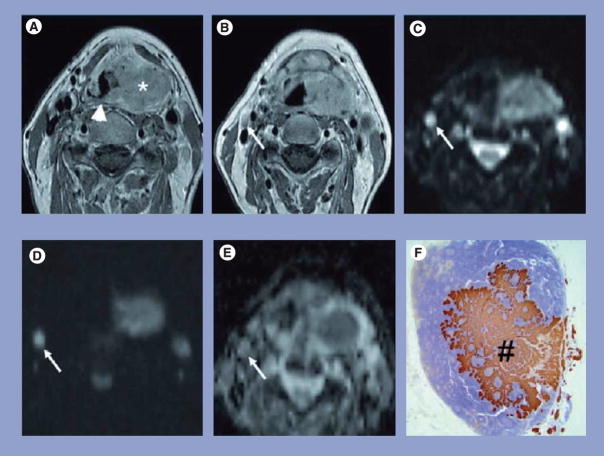
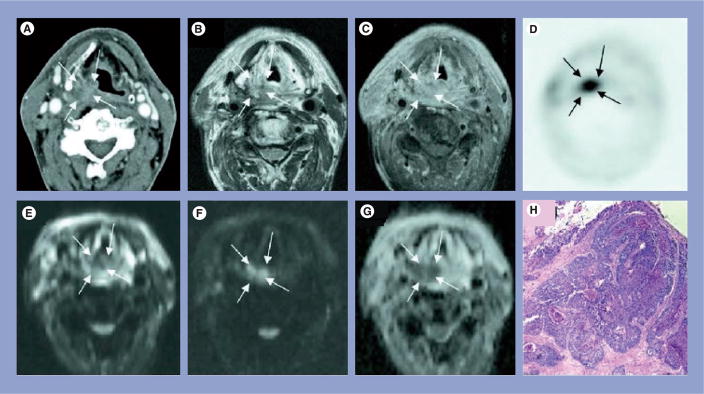
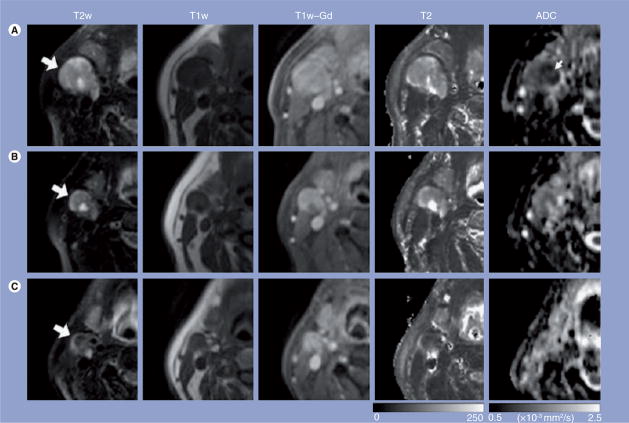
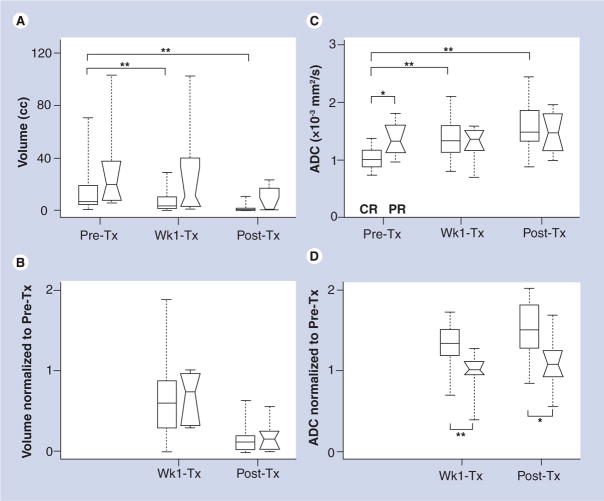
This article reviews the utility of diffusion-weighted imaging (DWI) in the diagnosis, prognosis and monitoring of treatment response in tumors arising in the head and neck region. The apparent diffusion coefficient (ADC) value, determined from DWI, can help in cancer staging and detection of subcentimeter nodal metastasis. The ADC value also discriminates carcinomas from lymphomas, benign lesions from malignant tumors and tumor necrosis from abscesses. Low pretreatment ADC values typically predict a favorable response to chemoradiation therapy. These promising reports indicate the potential of DWI as a potential biomarker for diagnosis and monitoring of treatment response in head and neck cancers. In view of the overlapping ADC values between different salivary gland tumors, care should be taken when interpreting these results and other imaging parameters should be considered for a better diagnosis. Susceptibility and motion-induced artifacts may sometimes degrade DWI image quality; however, novel techniques are being developed to overcome these drawbacks.
Figures
References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. - PubMed
-
- Pande P, Soni S, Kaur J, et al. Prognostic factors in betel and tobacco related oral cancer. Oral Oncol. 2002;38:491–499. - PubMed
-
- Argiris A, Haraf DJ, Kies MS, Vokes EE. Intensive concurrent chemoradiotherapy for head and neck cancer with 5-fluorouracil- and hydroxyurea-based regimens: reversing a pattern of failure. Oncologist. 2003;8:350–360. - PubMed
-
- Funk GF, Karnell LH, Robinson RA, et al. Presentation, treatment, and outcome of oral cavity cancer: a national cancer data base report. Head Neck. 2002;24:165–180. - PubMed
-
- Syrjanen S. Human papillomavirus infections and oral tumors. Med Microbiol Immunol. 2003;192:123–128. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical