

Sensory and motor peripheral nerve function and lower-extremity quadriceps strength: the health, aging and body composition study
- PMID: 19793163
- PMCID: PMC2899705
- DOI: 10.1111/j.1532-5415.2009.02487.x
Sensory and motor peripheral nerve function and lower-extremity quadriceps strength: the health, aging and body composition study
Abstract
Objectives: To determine whether sensory and motor nerve function is associated cross-sectionally with quadriceps or ankle dorsiflexion strength in an older community-based population.
Design: Cross-sectional analyses within a longitudinal cohort study.
Setting: Two U.S. clinical sites.
Participants: Two thousand fifty-nine Health, Aging and Body Composition Study (Health ABC) participants (49.5% male, 36.7% black, aged 73-82) in 2000/01.
Measurements: Quadriceps and ankle strength were measured using an isokinetic dynamometer. Sensory and motor peripheral nerve function in the legs and feet was assessed using 10-g and 1.4-g monofilaments, vibration threshold, and peroneal motor nerve conduction amplitude and velocity.
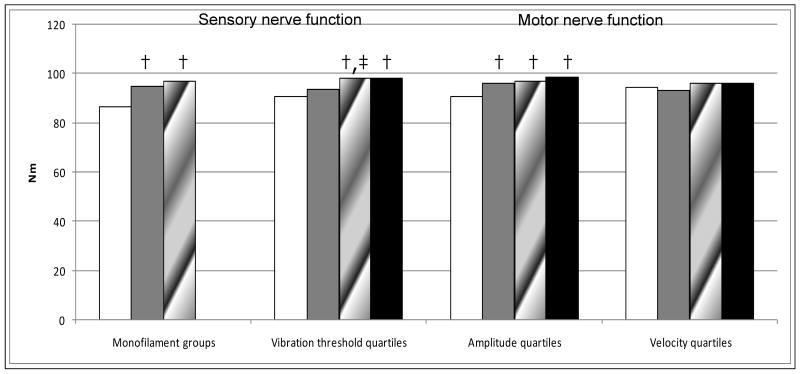
Results: Monofilament insensitivity, poorest vibration threshold quartile (>60 mu), and poorest motor nerve conduction amplitude quartile (<1.7 mV) were associated with 11%, 7%, and 8% lower quadriceps strength (all P<.01), respectively, than in the best peripheral nerve function categories in adjusted linear regression models. Monofilament insensitivity and lowest amplitude quartile were both associated with 17% lower ankle strength (P<.01). Multivariate analyses were adjusted for demographic characteristics, diabetes mellitus, body composition, lifestyle factors, and chronic health conditions and included all peripheral nerve measures in the same model. Monofilament insensitivity (beta=-7.19), vibration threshold (beta=-0.097), and motor nerve conduction amplitude (beta=2.01) each contributed independently to lower quadriceps strength (all P<.01). Monofilament insensitivity (beta=-5.29) and amplitude (beta=1.17) each contributed independently to lower ankle strength (all P<.01). Neither diabetes mellitus status nor lean mass explained the associations between peripheral nerve function and strength.
Conclusion: Reduced sensory and motor peripheral nerve function is related to poorer lower extremity strength in older adults, suggesting a mechanism for the relationship with lower extremity disability.
Conflict of interest statement
Conflict of Interest Disclosure: The authors report no conflict of interest.
Figures
References
-
- Evans W. Functional and metabolic consequences of sarcopenia. J Nutr. 1997;127:998S–1003S. - PubMed
-
- Baumgartner RN. Body composition in healthy aging. Ann N Y Acad Sci. 2000;904:437–448. - PubMed
-
- Goodpaster BH, Park SW, Harris TB, et al. The loss of skeletal muscle strength, mass, and quality in older adults: the Health, Aging and Body Composition Study. J Gerontol A Biol Sci Med Sci. 2006;61A:M1059–M1064. - PubMed
-
- Andersen JL. Muscle fiber type adaptation in the elderly human muscle. Scand J Med Sci Sports. 2003;13:40–47. - PubMed
-
- Baldereschi M, Inzitari M, Di Carlo A, Farchi G, Scafato E, Inzitari D, The ILSA Working Group Epidemiology of distal symmetrical neuropathies in the Italian elderly. Neurology. 2007;68:1460–1467. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
