

Review
doi: 10.1016/j.cps.2009.05.001.
The hypermetabolic response to burn injury and interventions to modify this response
Affiliations
- PMID: 19793553
- PMCID: PMC3776603
- DOI: 10.1016/j.cps.2009.05.001
Item in Clipboard
Review
The hypermetabolic response to burn injury and interventions to modify this response
Clin Plast Surg.
2009 Oct.
Abstract
Severe burn injury is followed by a profound hypermetabolic response that persists up to 24 months after injury. It is mediated by up to 50-fold elevations in plasma catecholamines, cortisol, and inflammatory cells that lead to whole-body catabolism, elevated resting energy expenditures, and multiorgan dysfunction. All of these metabolic and physiologic derangements prevent full rehabilitation and acclimatization of burn survivors back into society. Modulation of the response by early excision and grafting of burn wounds, thermoregulation, early and continuous enteral feeding with high-protein high-carbohydrate feedings, and pharmacologic treatments have markedly decreased morbidity.
Figures
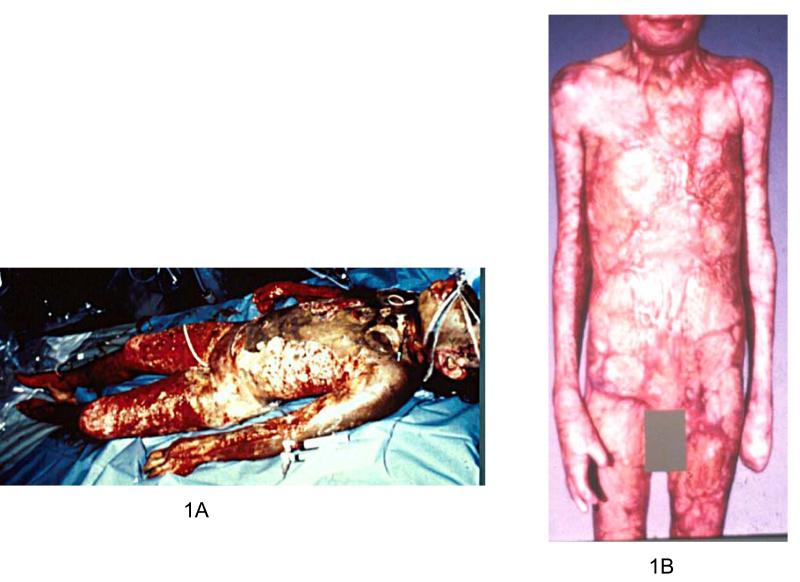
Adolescent pediatric burn patient with a 90% TBSA flame burn at admission (1A) and at one year (1B).

Metabolic rates of severely burned (≥ 40% TBSA) compared to normal non-burned children (previously unpublished). * Denotes significance at a p<0.05.
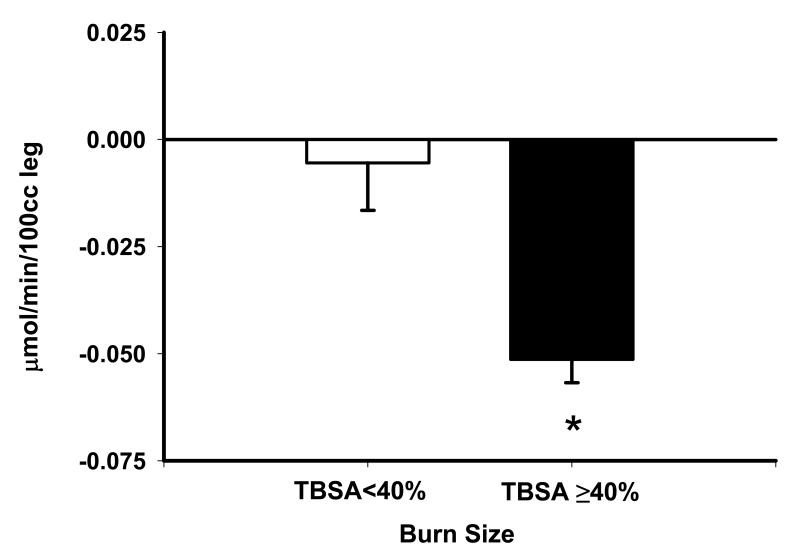
Effect of Burn Size on Net Muscle Protein Balance Control. Plotted on the graph is average ± standard error of the mean (SEM). The x-axis has two points, burns less than 40% TBSA, and burns ≥ 40% TBSA. * Denotes significance at p<0.05. Data was extrapolated from previously published data [17, 26]. The y-axis represents changes in net protein balance of muscle protein synthesis and breakdown induced by burn injury was measured by stable isotope studies using d5-phenyalanine infusion studies previously published [1, 11, 17, 26].
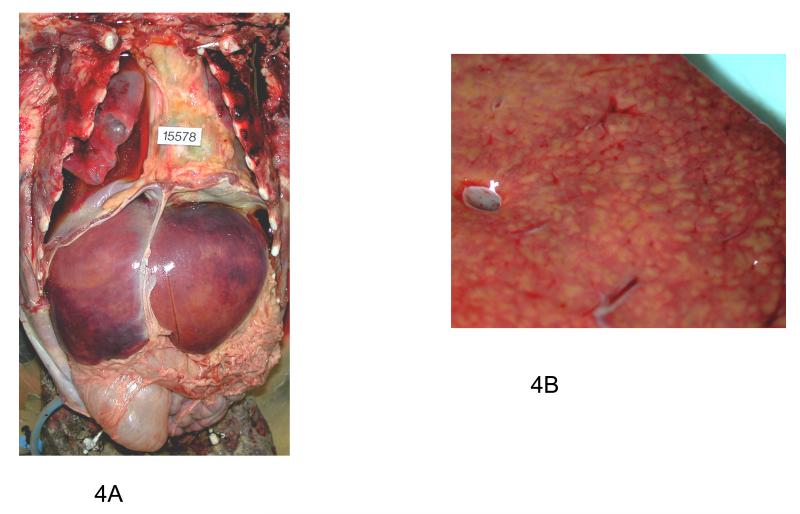
Gross Pathology of Hepatomegaly (4A) and Fatty Liver Infiltration (4B) post-burn. These pictures were taken post-mortem during the autopsy of a severely burned male pediatric patient (≥ 40% TBSA). Figure 4A is the macroscopic gross pathology of hepatomegaly post-burn. Figure 4B demonstrates the profound fatty liver infiltration seen post-burn.
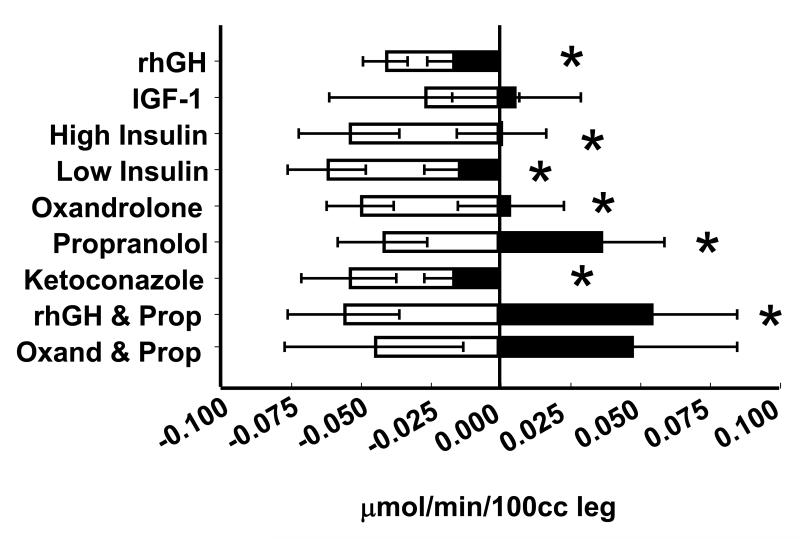
Relative efficacy of the different anabolic agents to improve muscle protein synthesis compared to standard of care alone. Changes in net protein balance of muscle protein synthesis and breakdown induced by burn injury was measured by stable isotope studies using d5-phenyalanine infusion studies previously published [1, 11, 17, 26, 95, 137, 138]. * Denotes significance of p<0.05. Graphs are averages ± SEM. White bars represent patients with burns ≥ 40% TBSA who received no anabolic agents. Black bars represent patients with burns ≥ 40% TBSA who were randomized to receive drug.
References
-
- Hart DW, Wolf SE, Mlcak R, et al. Persistence of muscle catabolism after severe burn. Surgery. 2000;128(2):312–9. - PubMed
-
- Rutan RL, Herndon DN. Growth delay in postburn pediatric patients. Arch Surg. 1990;125(3):392–5. - PubMed
-
- Yu YM, Tompkins RG, Ryan CM, et al. The metabolic basis of the increase of the increase in energy expenditure in severely burned patients. JPEN J Parenter Enteral Nutr. 1999;23(3):160–8. - PubMed
Publication types
MeSH terms
Grants and funding
- U54 GM062119/GM/NIGMS NIH HHS/United States
- 5R01GM56687-03/GM/NIGMS NIH HHS/United States
- R01 HD049471/HD/NICHD NIH HHS/United States
- 1P50GM60338-01/GM/NIGMS NIH HHS/United States
- M01 RR000073/RR/NCRR NIH HHS/United States
- R01 GM056687/GM/NIGMS NIH HHS/United States
- P50 GM060338/GM/NIGMS NIH HHS/United States
- R01 GM087285/GM/NIGMS NIH HHS/United States
- R01-HD049471/HD/NICHD NIH HHS/United States
- 2T32GM0825611/GM/NIGMS NIH HHS/United States
- U54/GM62119/GM/NIGMS NIH HHS/United States
- T32 GM008256/GM/NIGMS NIH HHS/United States
- R01-GM56687/GM/NIGMS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
