

Admission chemokine (C-C motif) ligand 4 levels predict survival in pediatric septic shock
- PMID: 19794326
- PMCID: PMC2837132
- DOI: 10.1097/PCC.0b013e3181b8076c
Admission chemokine (C-C motif) ligand 4 levels predict survival in pediatric septic shock
Abstract
Objective: Stratification with an effective outcome biomarker could improve the design of interventional trials in pediatric septic shock. The objective of this study was to test the usefulness of chemokine (C-C motif) ligand 4 as an outcome biomarker for mortality in pediatric septic shock.
Design: A cross-sectional, observational study.
Setting: Eighteen pediatric intensive care units in the United States.
Patients: One hundred fifty-six pediatric patients with septic shock.
Interventions: Serum samples were obtained within 24 hrs of admission to the pediatric intensive care unit. Serum levels of chemokine (C-C motif) ligand 4 were measured by enzyme-linked immunosorbent assay and compared with mortality in a training set of 34 patients. These data were used to generate a cutoff value whose usefulness was evaluated through prospective application-without post hoc modification-to a larger validation set of 122 patients.
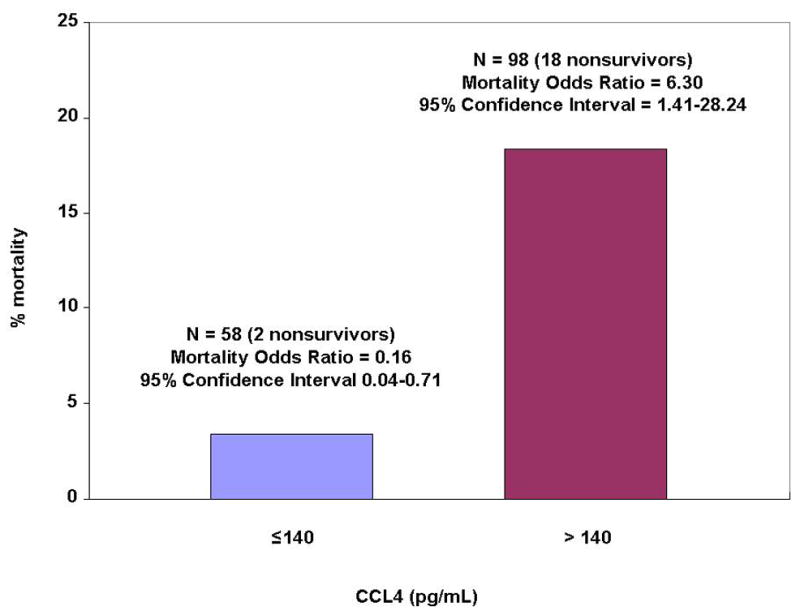
Measurements and main results: On inspection of the training set data, a cutoff value of 140 pg/mL was chosen. When applied to the validation set, serum chemokine (C-C motif) ligand 4 levels >140 pg/mL yielded a sensitivity of 92% and a specificity of 40% for mortality. A serum level of < or =140 pg/mL had a negative predictive value for mortality of 98%.
Conclusions: A serum level of chemokine (C-C motif) ligand 4 of < or =140 pg/mL, when obtained within 24 hrs of admission, predicts a very high likelihood of survival in pediatric septic shock. Exclusion of patients with a chemokine (C-C motif) ligand 4 level of < or =140 pg/mL from interventional clinical trials in pediatric septic shock could create a study population in which survival benefit from the study agent could be more readily demonstrated.
Figures



Comment in
-
It's not cherry-picking, it's bridging the gap.Pediatr Crit Care Med. 2010 Mar;11(2):304-5. doi: 10.1097/PCC.0b013e3181cbdd48. Pediatr Crit Care Med. 2010. PMID: 20216178 No abstract available.
References
-
- Watson RS, Carcillo JA, Linde-Zwirble WT, et al. The epidemiology of severe sepsis in children in the United States. Am J Respir Crit Care Med. 2003;167:695–701. - PubMed
-
- Watson RS, Carcillo JA. Scope and epidemiology of pediatric sepsis. Pediatr Crit Care Med. 2005;6:S3–5. - PubMed
-
- Dombrovskiy VY, Martin AA, Sunderram J, Paz HL. Rapid increase in hospitalization and mortality rates for severe sepsis in the United States: a trend analysis from 1993 to 2003. Crit Care Med. 2007;35:1244–50. - PubMed
-
- Marshall JC, Vincent J, Fink MP, Cook DJ, et al. Measures, markers, and mediators: toward a staging system for clinical sepsis. A report of the Fifth Toronto Sepsis Roundtable, Toronto, Ontario, Canada, October 25–26, 2000. Crit Care Med. 2003;31:1560–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
