Comparison of photocoagulation with combined intravitreal triamcinolone for diabetic macular edema
- PMID: 19794940
- PMCID: PMC2739972
- DOI: 10.3341/kjo.2009.23.3.153
Comparison of photocoagulation with combined intravitreal triamcinolone for diabetic macular edema
Abstract
Purpose: To compare the efficacy between macular laser grid (MLG) photocoagulation and MLG plus intravitreal triamcinolone acetonide (IVTA; MLG+IVTA) therapy in diabetic macular edema (DME) patients.
Methods: A prospective, randomized, clinical trial was conducted of DME patients. A total of 60 eyes (54 patients) affected by DME were observed for a minimum of 6 months. Thirty eyes of 28 patients who received MLG treatment and 30 eyes of 26 patients who received the combined MLG+IVTA treatment were included in the study. Main outcome measures were BCVA and central macular thickness (CMT) as measured by optical coherence tomography (OCT) at 1, 3, and 6 months after treatment. Additionally, the authors examined retrospectively 20 eyes of 20 patients who were treated with only IVTA and compared with the 2 groups (MLG group and MLG+IVTA group).
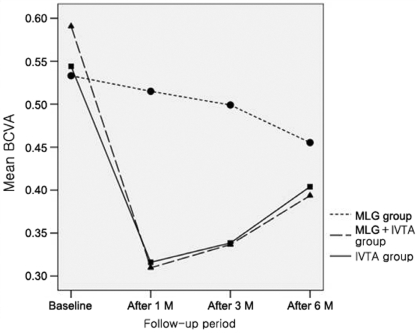
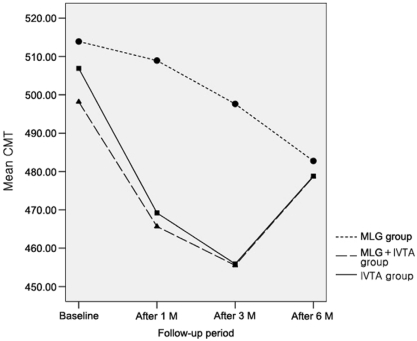
Results: Baseline BCVA was 0.53 + or - 0.32 and CMT was 513.9 + or - 55.1 microm in the MLG group. At 1 and 3 months after treatment, the MLG group showed no significant improvement of BCVA and CMT, although there was significant improvement after 6 months. In the MLG+IVTA group, the baseline BCVA was 0.59 + or - 0.29 and CMT was 498.2 + or - 19.8 microm. After treatment, significant improvement of BCVA and CMT was observed at all follow-up time periods. When comparing the MLG group with the MLG+IVTA group, the latter had better results after 1 and 3 months, although at 6 months, there was no significant difference of BCVA and CMT between the 2 groups. Additionally, the IVTA group showed more improvement than the MLG group at 1 and 3 months but showed no significant difference at 6 months. In addition, the IVTA group showed no significant difference with the MLG+IVTA group at all follow-up time periods.
Conclusions: For DME patients, the combined MLG+IVTA treatment had a better therapeutic effect than the MLG treatment for improving BCVA and CMT at the early follow-up time periods. IVTA treatment alone could be an additional alternative therapeutic option to combined therapy.
Keywords: Central macular thickness; Diabetic macular edema; Diabetic retinopathy; Intravitreal triamcinolone acetonide injection; Macular laser grid photocoagulation.
Figures
Similar articles
-
Intravitreal triamcinolone as an adjunct to standard laser therapy in coexisting high-risk proliferative diabetic retinopathy and clinically significant macular edema.Retina. 2010 Feb;30(2):254-9. doi: 10.1097/IAE.0b013e3181b4f125. Retina. 2010. PMID: 20057344 Clinical Trial.
-
Efficacy of intravitreal triamcinolone for the treatment of macular edema secondary to branch retinal vein occlusion in eyes with or without grid laser photocoagulation.Retina. 2008 Mar;28(3):465-72. doi: 10.1097/IAE.0b013e318154b9d1. Retina. 2008. PMID: 18327140
-
Intravitreal triamcinolone compared with macular laser grid photocoagulation for the treatment of cystoid macular edema.Am J Ophthalmol. 2005 Oct;140(4):695-702. doi: 10.1016/j.ajo.2005.05.021. Am J Ophthalmol. 2005. PMID: 16226521 Clinical Trial.
-
Efficacy and safety of triamcinolone acetonide injection combined with laser photocoagulation in the treatment of diabetic macular edema: a systematic review and meta-analysis.Ann Palliat Med. 2021 Dec;10(12):12467-12477. doi: 10.21037/apm-21-3274. Ann Palliat Med. 2021. PMID: 35016410
-
Intravitreal triamcinolone acetonide injection for treatment of refractory diabetic macular edema: a systematic review.Ophthalmology. 2009 May;116(5):902-11; quiz 912-3. doi: 10.1016/j.ophtha.2009.02.002. Ophthalmology. 2009. PMID: 19410949
Cited by
-
Current treatments in diabetic macular oedema: systematic review and meta-analysis.BMJ Open. 2013 Mar 1;3(3):e002269. doi: 10.1136/bmjopen-2012-002269. BMJ Open. 2013. PMID: 23457327 Free PMC article.
-
Macular laser photocoagulation with or without intravitreal triamcinolone pretreatment for diabetic macular edema: a result from five randomized controlled trials.Int J Ophthalmol. 2016 Jan 18;9(1):132-8. doi: 10.18240/ijo.2016.01.22. eCollection 2016. Int J Ophthalmol. 2016. PMID: 26949623 Free PMC article.
-
Current approaches to the management of diabetic retinopathy and diabetic macular oedema.Drugs. 2010 Nov 12;70(16):2171-200. doi: 10.2165/11538130-000000000-00000. Drugs. 2010. PMID: 20964459 Review.
-
Efficacy of different routes of triamcinolone acetonide administration on macular edema: A systematic review and network meta-analysis.PLoS One. 2025 Jan 24;20(1):e0317782. doi: 10.1371/journal.pone.0317782. eCollection 2025. PLoS One. 2025. PMID: 39854565 Free PMC article.
-
Five-month observation of persistent diabetic macular edema after intravitreal injection of Ozurdex implant.Mediators Inflamm. 2014;2014:364143. doi: 10.1155/2014/364143. Epub 2014 Feb 10. Mediators Inflamm. 2014. PMID: 24659860 Free PMC article.
References
-
- Ryan Stephen J. Nonproliferative diabetic retinopathy. In: Chew Emily Y., Ferris Fredrick L., III, editors. Retina. 4th ed. v. 2. New York: Mosby, Elsevier Inc.; 2006. chap. 67.
-
- Early Treatment Diabetic Retinopathy Study Research Group. Photocoagulation for diabetic macular edema. Early Treatment Diabetic Retinopathy Study Report Number 1. Arch Ophthalmol. 1985;103:1796–1806. - PubMed
-
- Early Treatment Diabetic Retinopathy Study Research Group. Treatment techniques and clinical guidelines for photocoagulation of diabetic macular edema. Early Treatment Diabetic Retinopathy Study Report Number 2. Ophthalmology. 1987;94:761–774. - PubMed
-
- Early Treatment Diabetic Retinopathy Study Research Group. Focal photocoagulation treatment of diabetic macular edema. Relationship of treatment effect to fluorescein angiographic and other retinal characteristics at baseline: ETDRS report no. 19. Arch Ophthalmol. 1995;113:1144–1155. - PubMed
-
- Martidis A, Duker JS, Greenberg PB, et al. Intravitreal triamcinolone for refractory diabetic macular edema. Ophthalmology. 2002;109:920–927. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical