

Fall prevention with supplemental and active forms of vitamin D: a meta-analysis of randomised controlled trials
- PMID: 19797342
- PMCID: PMC2755728
- DOI: 10.1136/bmj.b3692
Fall prevention with supplemental and active forms of vitamin D: a meta-analysis of randomised controlled trials
Abstract
Objective: To test the efficacy of supplemental vitamin D and active forms of vitamin D with or without calcium in preventing falls among older individuals.
Data sources: We searched Medline, the Cochrane central register of controlled trials, BIOSIS, and Embase up to August 2008 for relevant articles. Further studies were identified by consulting clinical experts, bibliographies, and abstracts. We contacted authors for additional data when necessary. Review methods Only double blind randomised controlled trials of older individuals (mean age 65 years or older) receiving a defined oral dose of supplemental vitamin D (vitamin D(3) (cholecalciferol) or vitamin D(2) (ergocalciferol)) or an active form of vitamin D (1alpha-hydroxyvitamin D(3) (1alpha-hydroxycalciferol) or 1,25-dihydroxyvitamin D(3) (1,25-dihydroxycholecalciferol)) and with sufficiently specified fall assessment were considered for inclusion.
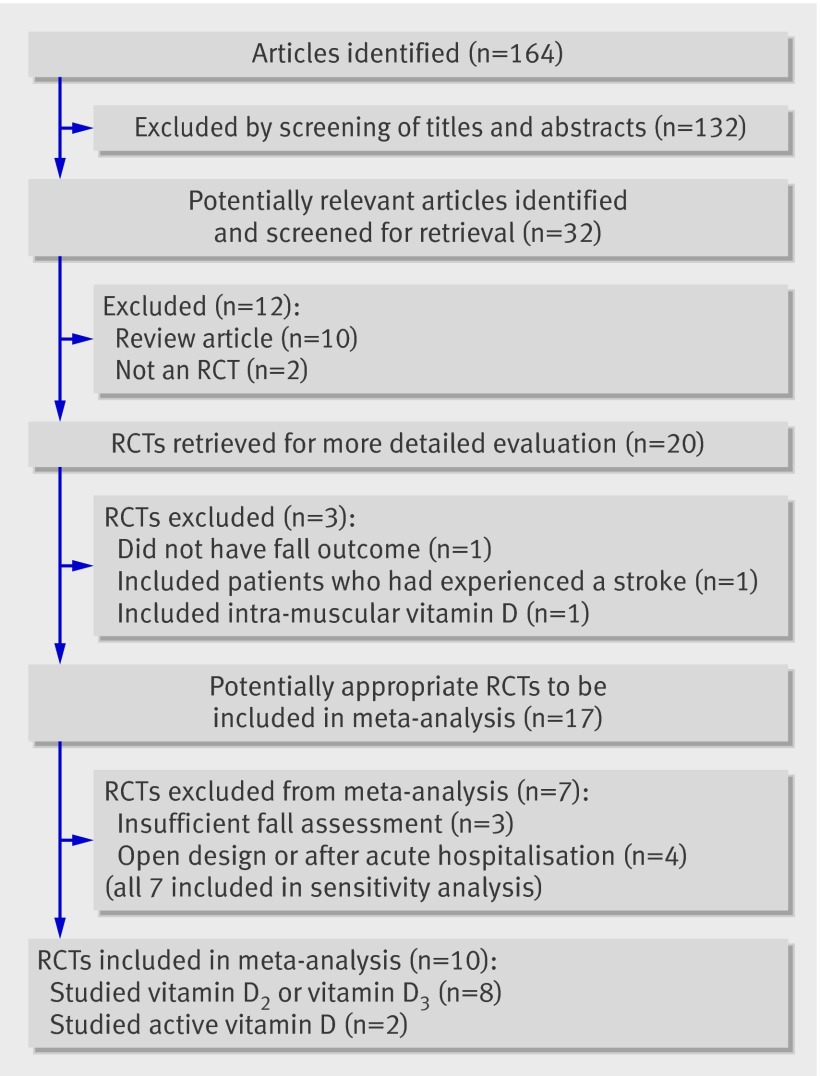
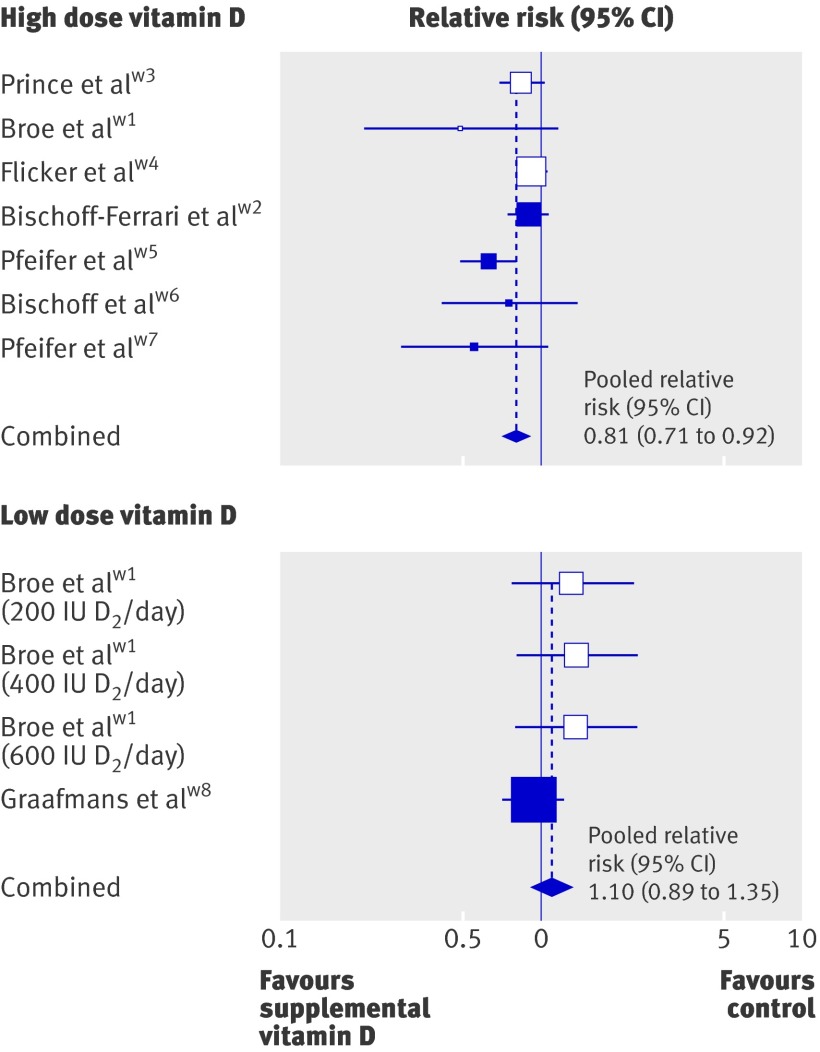
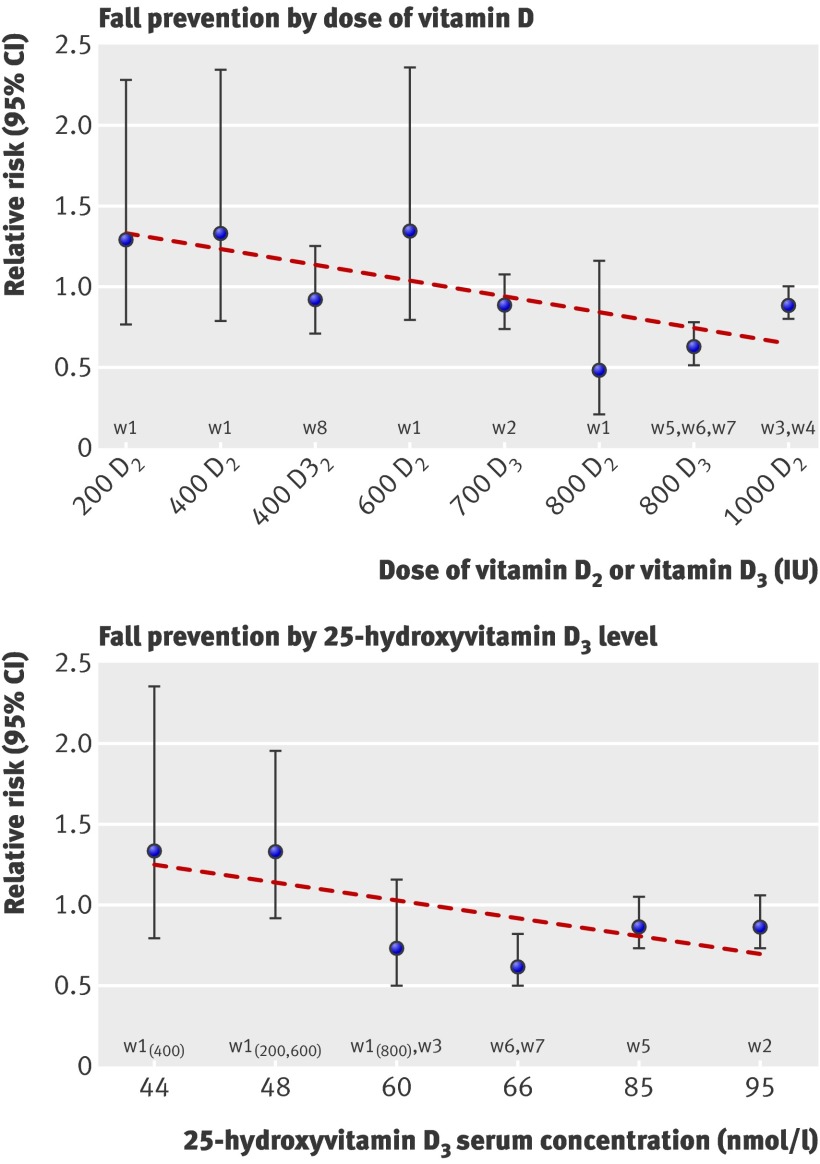
Results: Eight randomised controlled trials (n=2426) of supplemental vitamin D met our inclusion criteria. Heterogeneity among trials was observed for dose of vitamin D (700-1000 IU/day v 200-600 IU/day; P=0.02) and achieved 25-hydroxyvitamin D(3) concentration (25(OH)D concentration: <60 nmol/l v >or=60 nmol/l; P=0.005). High dose supplemental vitamin D reduced fall risk by 19% (pooled relative risk (RR) 0.81, 95% CI 0.71 to 0.92; n=1921 from seven trials), whereas achieved serum 25(OH)D concentrations of 60 nmol/l or more resulted in a 23% fall reduction (pooled RR 0.77, 95% CI 0.65 to 0.90). Falls were not notably reduced by low dose supplemental vitamin D (pooled RR 1.10, 95% CI 0.89 to 1.35; n=505 from two trials) or by achieved serum 25-hydroxyvitamin D concentrations of less than 60 nmol/l (pooled RR 1.35, 95% CI 0.98 to 1.84). Two randomised controlled trials (n=624) of active forms of vitamin D met our inclusion criteria. Active forms of vitamin D reduced fall risk by 22% (pooled RR 0.78, 95% CI 0.64 to 0.94).
Conclusions: Supplemental vitamin D in a dose of 700-1000 IU a day reduced the risk of falling among older individuals by 19% and to a similar degree as active forms of vitamin D. Doses of supplemental vitamin D of less than 700 IU or serum 25-hydroxyvitamin D concentrations of less than 60 nmol/l may not reduce the risk of falling among older individuals.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Vitamin D and falls. Time for a moratorium on vitamin D meta-analyses?BMJ. 2009 Oct 28;339:b4394. doi: 10.1136/bmj.b4394. BMJ. 2009. PMID: 19864356 No abstract available.
-
Vitamin D and falls. Information on harm is missing.BMJ. 2009 Oct 28;339:b4395. doi: 10.1136/bmj.b4395. BMJ. 2009. PMID: 19864357 No abstract available.
-
ACP Journal Club. Review: high-dose oral vitamin D supplements and active vitamin D prevent falls in older persons.Ann Intern Med. 2010 Jan 19;152(2):JC1-3. doi: 10.7326/0003-4819-152-2-201001190-02003. Ann Intern Med. 2010. PMID: 20083818 No abstract available.
-
Fall prevention with vitamin D. Clarifications needed, please.BMJ. 2011 May 3;342:d2602. doi: 10.1136/bmj.d2602. BMJ. 2011. PMID: 21540263 No abstract available.
References
-
- Blake AJ, Morgan K, Bendall MJ, Dallosso H, Ebrahim SB, Arie TH, et al. Falls by elderly people at home: prevalence and associated factors. Age Ageing 1988;17:365-72. - PubMed
-
- Graafmans WC, Ooms ME, Hofstee HM, Bezemer PD, Bouter LM, Lips P. Falls in the elderly: a prospective study of risk factors and risk profiles. Am J Epidemiol 1996;143:1129-36. - PubMed
-
- Tinetti ME, Speechley M, Ginter SF. Risk factors for falls among elderly persons living in the community. N Engl J Med 1988;319:1701-7. - PubMed
-
- Bischoff HA, Stahelin HB, Dick W, Akos R, Knecht M, Salis C, et al. Effects of vitamin D and calcium supplementation on falls: a randomized controlled trial. J Bone Miner Res 2003;18:343-51. - PubMed
-
- Bischoff-Ferrari HA, Borchers M, Gudat F, Durmuller U, Stahelin HB, Dick W. Vitamin D receptor expression in human muscle tissue decreases with age. J Bone Miner Res 2004;19:265-9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous