

Acute coronary syndromes: diagnosis and management, part I
- PMID: 19797781
- PMCID: PMC2755812
- DOI: 10.4065/84.10.917
Acute coronary syndromes: diagnosis and management, part I
Abstract
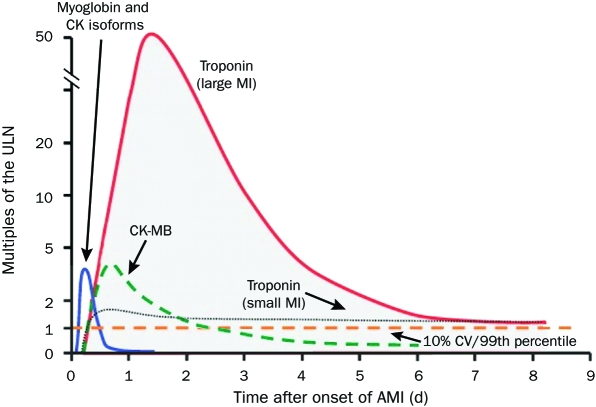
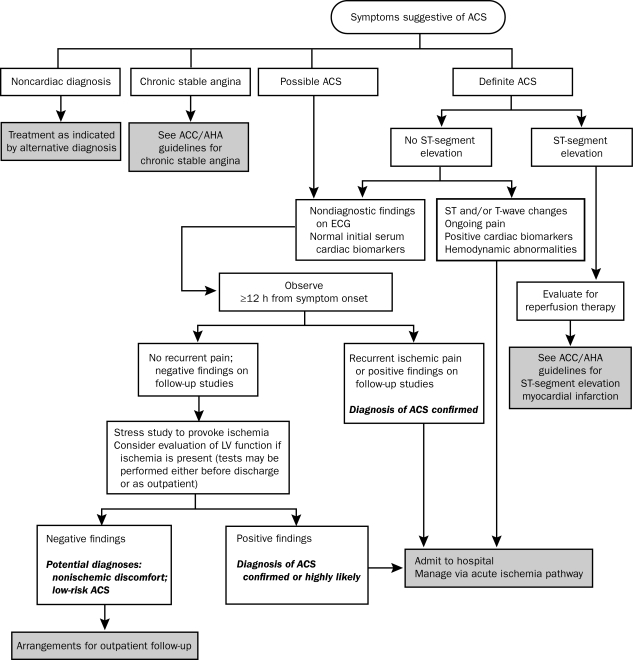
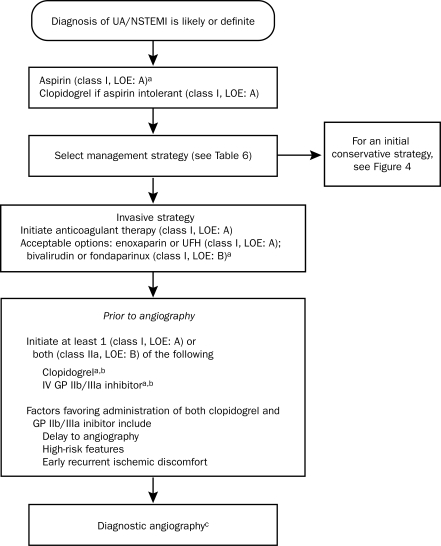
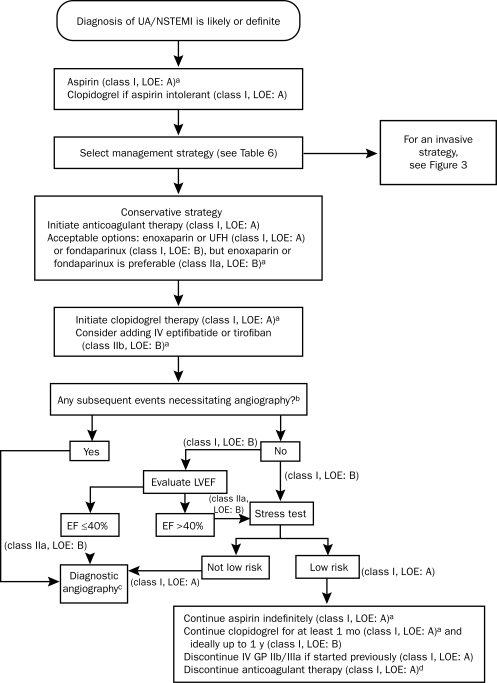
The term acute coronary syndrome (ACS) refers to any group of clinical symptoms compatible with acute myocardial ischemia and includes unstable angina (UA), non-ST-segment elevation myocardial infarction (NSTEMI), and ST-segment elevation myocardial infarction (STEMI). These high-risk manifestations of coronary atherosclerosis are important causes of the use of emergency medical care and hospitalization in the United States. A quick but thorough assessment of the patient's history and findings on physical examination, electrocardiography, radiologic studies, and cardiac biomarker tests permit accurate diagnosis and aid in early risk stratification, which is essential for guiding treatment. High-risk patients with UA/NSTEMI are often treated with an early invasive strategy involving cardiac catheterization and prompt revascularization of viable myocardium at risk. Clinical outcomes can be optimized by revascularization coupled with aggressive medical therapy that includes anti-ischemic, antiplatelet, anticoagulant, and lipid-lowering drugs. Evidence-based guidelines provide recommendations for the management of ACS; however, therapeutic approaches to the management of ACS continue to evolve at a rapid pace driven by a multitude of large-scale randomized controlled trials. Thus, clinicians are frequently faced with the problem of determining which drug or therapeutic strategy will achieve the best results. This article summarizes the evidence and provides the clinician with the latest information about the pathophysiology, clinical presentation, and risk stratification of ACS and the management of UA/NSTEMI.
Figures
References
-
- Lloyd-Jones D, Adams R, Carnethon M, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics—2009 update. a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee [published correction appears in Circulation. 2009;119(3):e182] Circulation 2009January27;119(3):480-486 Epub 2008 Dec 15 - PubMed
-
- Fuster V, Badimon L, Cohen M, Ambrose JA, Badimon JJ, Chesebro J. Insights into the pathogenesis of acute ischemic syndromes. Circulation 1988;77(6):1213-1220 - PubMed
-
- Fuster V, Badimon L, Badimon JJ, Chesebro JH. The pathogenesis of coronary artery disease and the acute coronary syndromes (2). N Engl J Med. 1992;326(5):310-318 - PubMed
-
- Libby P. Current concepts of the pathogenesis of the acute coronary syndromes. Circulation 2001;104(3):365-372 - PubMed
-
- Corti R, Fuster V, Badimon JJ, Hutter R, Fayad ZA. New understanding of atherosclerosis (clinically and experimentally) with evolving MRI technology in vivo. Ann N Y Acad Sci. 2001;947:181-195 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
