

Continued cytoadherence of Plasmodium falciparum infected red blood cells after antimalarial treatment
- PMID: 19800372
- PMCID: PMC2814047
- DOI: 10.1016/j.molbiopara.2009.09.007
Continued cytoadherence of Plasmodium falciparum infected red blood cells after antimalarial treatment
Abstract
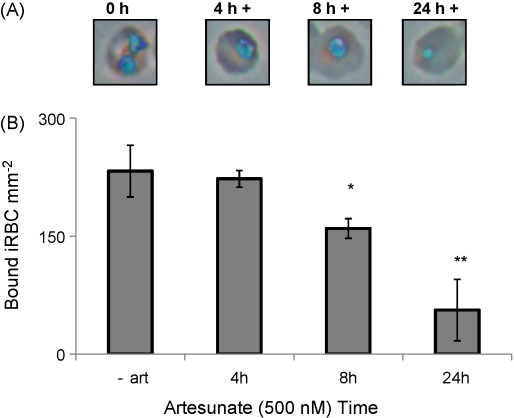
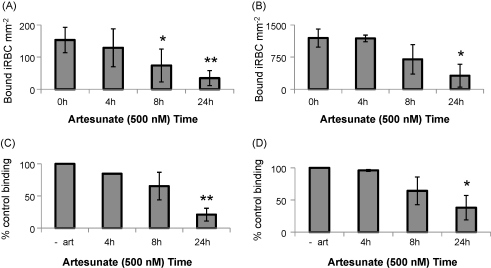
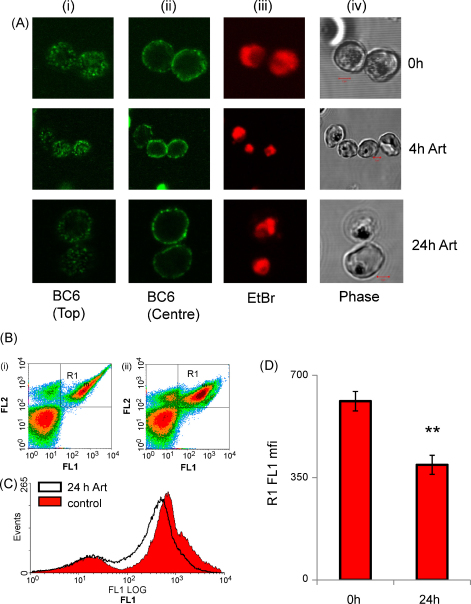
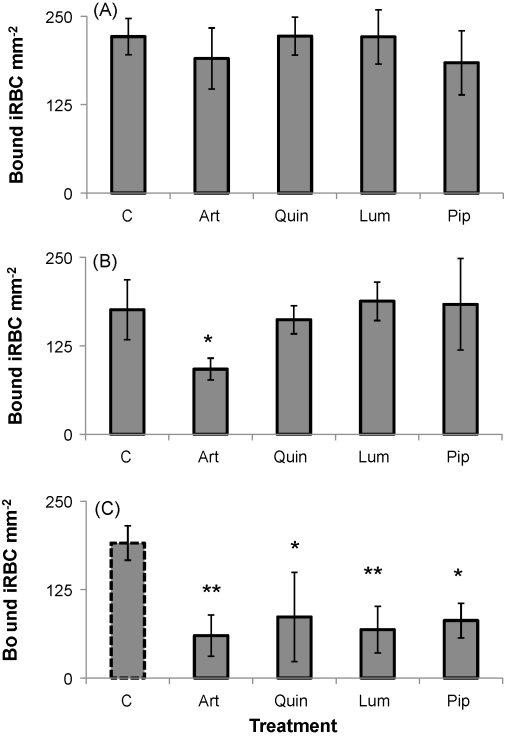
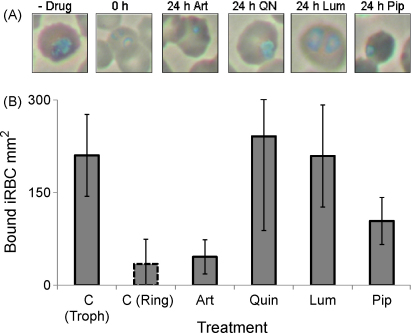
Development of severe disease in Plasmodium falciparum malaria infection is thought to be, at least in part, due to the sequestration of trophozoite-stage infected red blood cells in the microvasculature. The process of cytoadherence is mediated by binding of the parasite protein PfEMP-1 on the surface of infected red blood cells to endothelial cell receptors. Although antimalarial treatments rapidly kill parasites, significant mortality is still seen in severe malaria, particularly within 24h of hospital admission. We find that cytoadherence of infected red blood cells continues for several hours after killing of the parasite by antimalarials; after 24h treatment using a range of antimalarials binding is approximately one-third the level of untreated parasite cultures. This is consistent with the maintained presence of PfEMP-1 on the surface of drug-treated infected red blood cells. A specific advantage of artesunate over other treatments tested is seen on addition of this drug to younger ring stage parasites, which do not mature to the cytoadherent trophozoite-stage. These findings show that cytoadherence, a potential pathogenic property of P. falciparum infected red blood cells, continues long after the parasite has been killed. These data support the development of adjunctive therapies to reverse the pathophysiological consequences of cytoadherence.
Figures
Similar articles
-
Febrile temperatures induce cytoadherence of ring-stage Plasmodium falciparum-infected erythrocytes.Proc Natl Acad Sci U S A. 2002 Sep 3;99(18):11825-9. doi: 10.1073/pnas.172398999. Epub 2002 Aug 12. Proc Natl Acad Sci U S A. 2002. PMID: 12177447 Free PMC article.
-
Broad inhibition of plasmodium falciparum cytoadherence by (+)-epigallocatechin gallate.Malar J. 2011 Dec 1;10:348. doi: 10.1186/1475-2875-10-348. Malar J. 2011. PMID: 22132804 Free PMC article.
-
Cytoadherence phenotype of Plasmodium falciparum-infected erythrocytes is associated with specific pfemp-1 expression in parasites from children with cerebral malaria.Malar J. 2014 Aug 25;13:333. doi: 10.1186/1475-2875-13-333. Malar J. 2014. PMID: 25156105 Free PMC article.
-
The Plasmodium falciparum-infected red blood cell.Int J Biochem Cell Biol. 2011 Jun;43(6):839-42. doi: 10.1016/j.biocel.2011.03.012. Epub 2011 Mar 31. Int J Biochem Cell Biol. 2011. PMID: 21458590 Review.
-
The role of ICAM-1 in Plasmodium falciparum cytoadherence.Eur J Cell Biol. 2005 Jan;84(1):15-27. doi: 10.1016/j.ejcb.2004.09.002. Eur J Cell Biol. 2005. PMID: 15724813 Review.
Cited by
-
Macrolides rapidly inhibit red blood cell invasion by the human malaria parasite, Plasmodium falciparum.BMC Biol. 2015 Jul 18;13:52. doi: 10.1186/s12915-015-0162-0. BMC Biol. 2015. PMID: 26187647 Free PMC article.
-
Disrupting malaria parasite AMA1-RON2 interaction with a small molecule prevents erythrocyte invasion.Nat Commun. 2013;4:2261. doi: 10.1038/ncomms3261. Nat Commun. 2013. PMID: 23907321 Free PMC article.
-
The fluid management of adults with severe malaria.Crit Care. 2014 Nov 21;18(6):642. doi: 10.1186/s13054-014-0642-6. Crit Care. 2014. PMID: 25629462 Free PMC article.
-
Structure-function-immunogenicity studies of PfEMP1 domain DBL2βPF11_0521, a malaria parasite ligand for ICAM-1.PLoS One. 2013 Apr 12;8(4):e61323. doi: 10.1371/journal.pone.0061323. Print 2013. PLoS One. 2013. PMID: 23593462 Free PMC article.
-
Small Molecule Compounds Identified from Mixture-Based Library Inhibit Binding between Plasmodium falciparum Infected Erythrocytes and Endothelial Receptor ICAM-1.Int J Mol Sci. 2021 May 26;22(11):5659. doi: 10.3390/ijms22115659. Int J Mol Sci. 2021. PMID: 34073419 Free PMC article.
References
-
- Taylor T.E., Fu W.J., Carr R.A. Differentiating the pathologies of cerebral malaria by postmortem parasite counts. Nat Med. 2004;10(2):143–145. - PubMed
-
- Chakravorty S.J., Hughes K.R., Craig A.G. Host response to cytoadherence in Plasmodium falciparum. Biochem Soc Trans. 2008;36(Pt 2):221–228. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
