

Cardiac T2* magnetic resonance for prediction of cardiac complications in thalassemia major
- PMID: 19801505
- PMCID: PMC2784198
- DOI: 10.1161/CIRCULATIONAHA.109.874487
Cardiac T2* magnetic resonance for prediction of cardiac complications in thalassemia major
Abstract
Background: The goal of this study was to determine the predictive value of cardiac T2* magnetic resonance for heart failure and arrhythmia in thalassemia major.
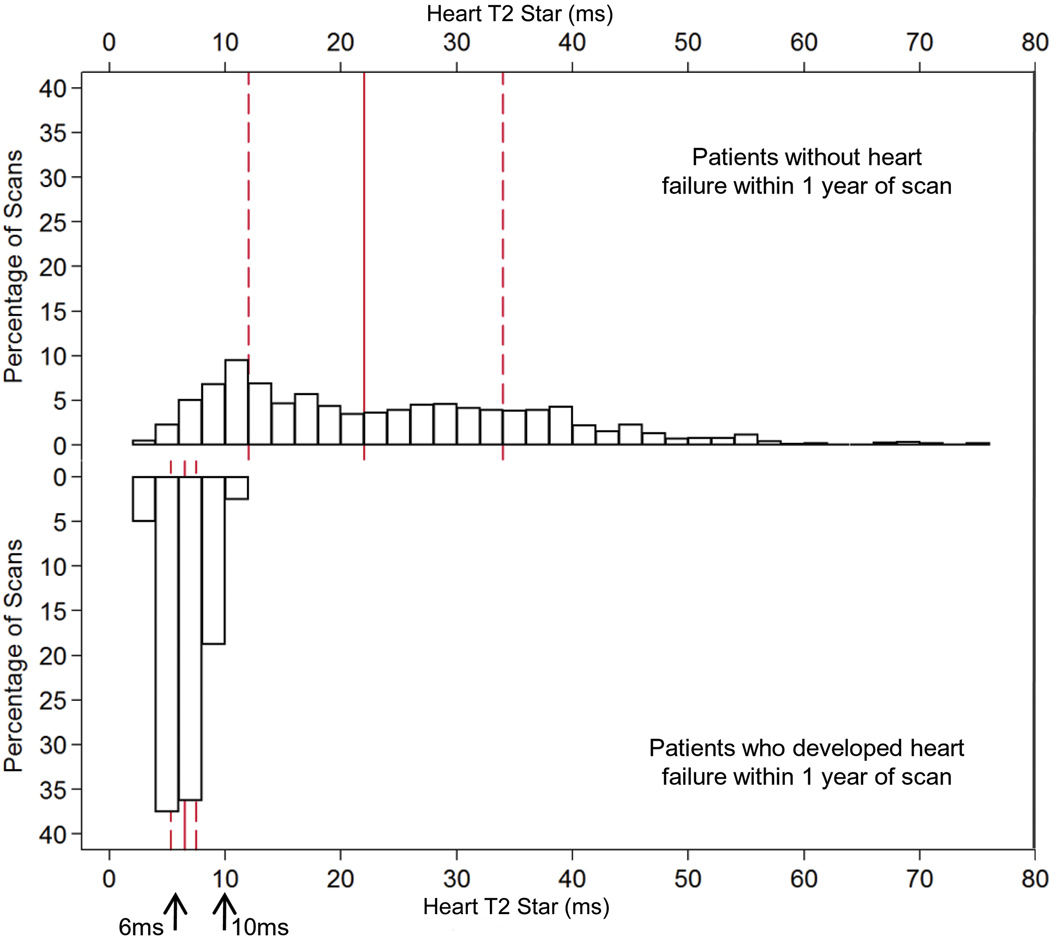
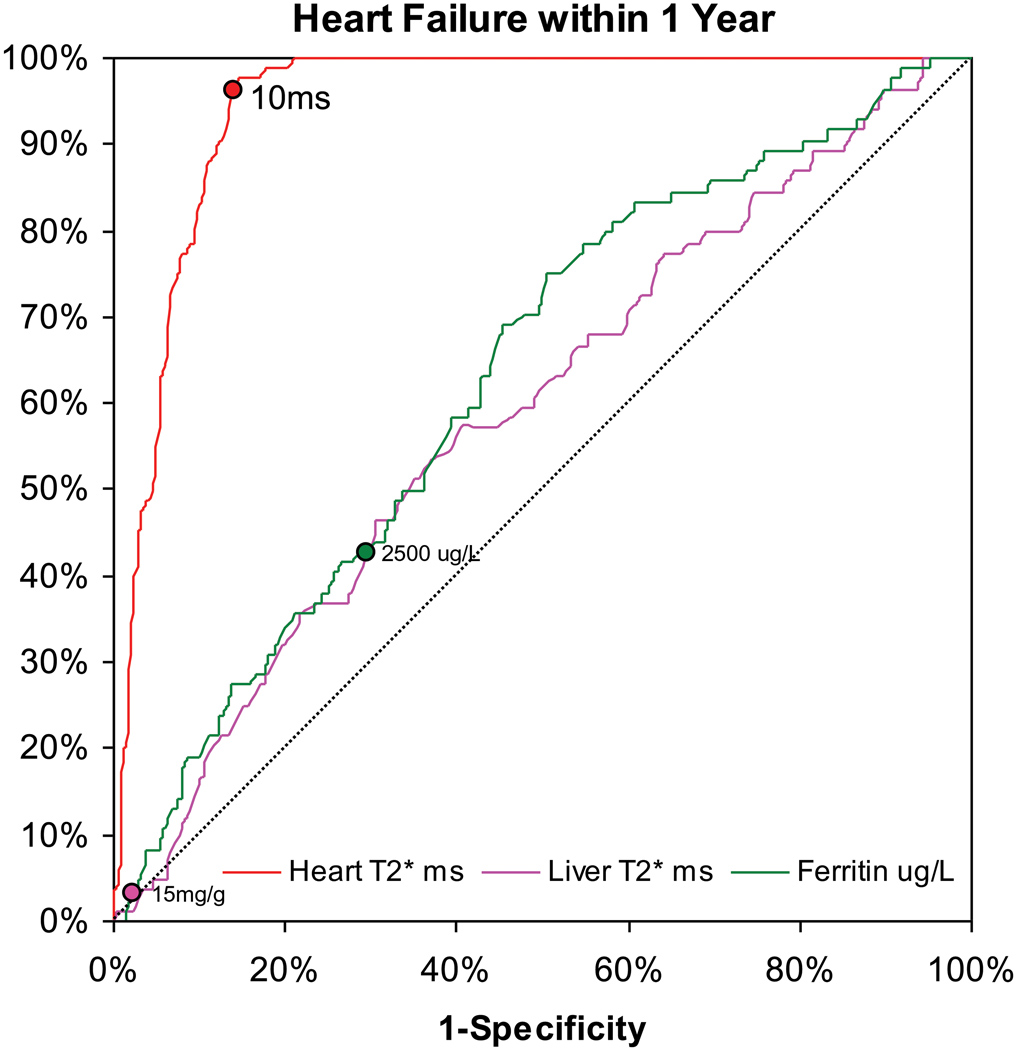
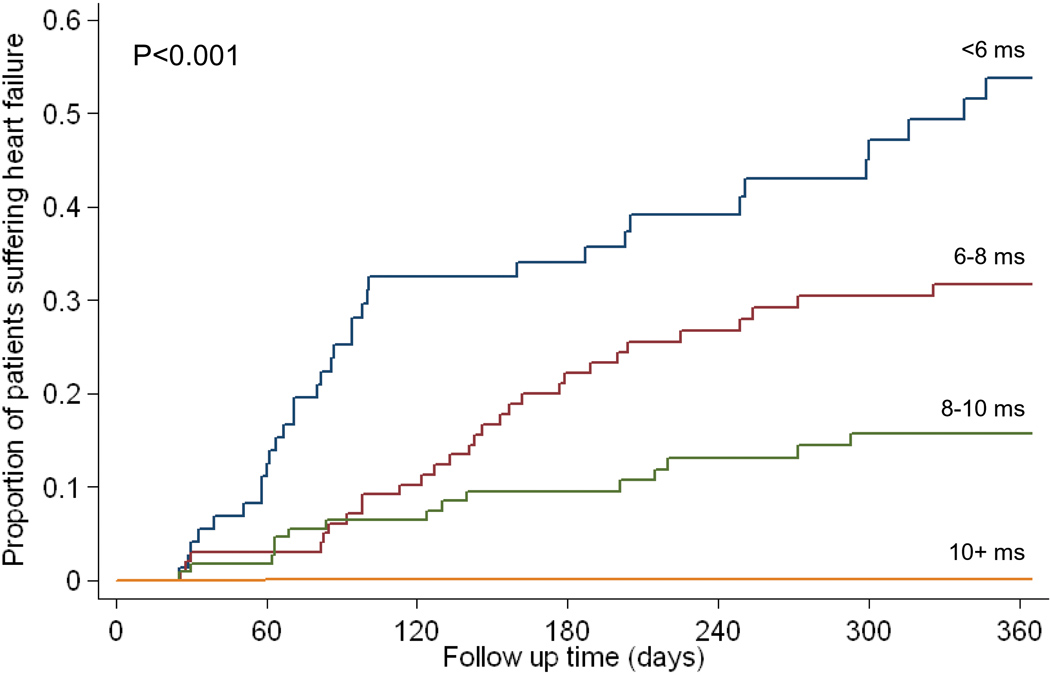
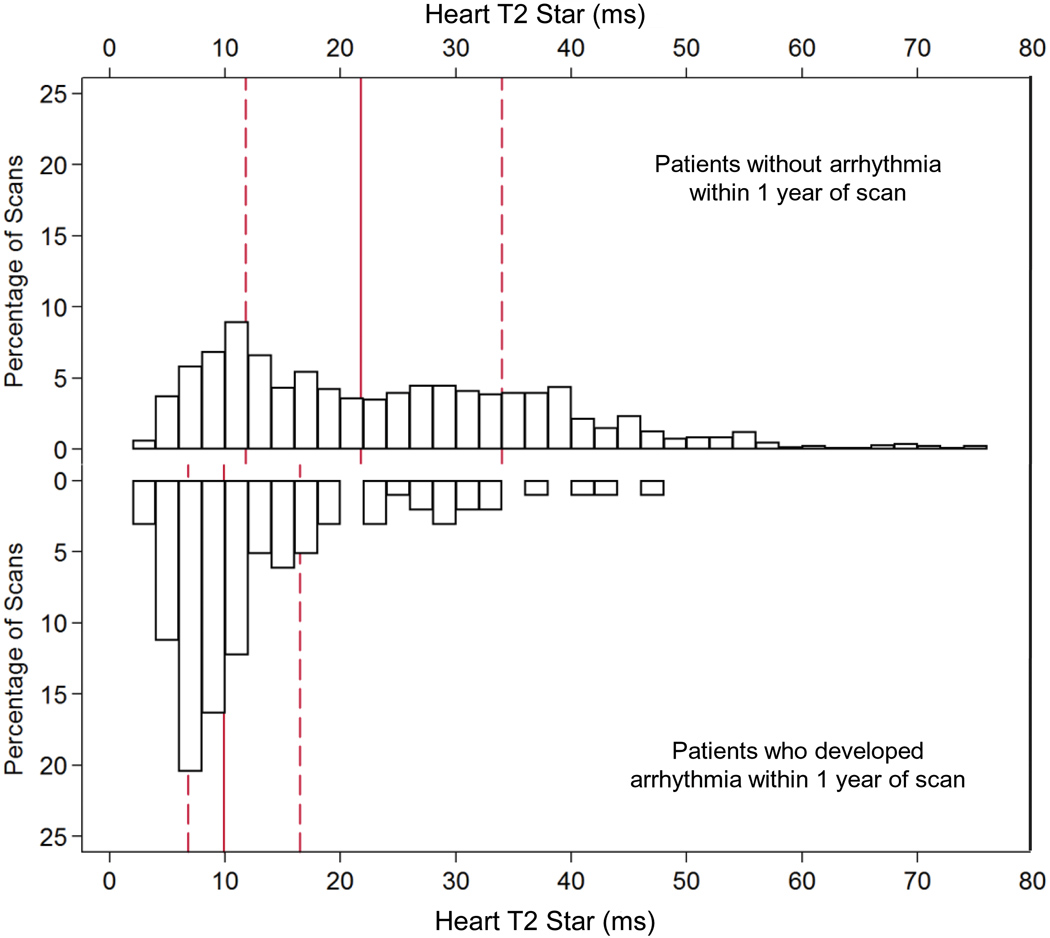
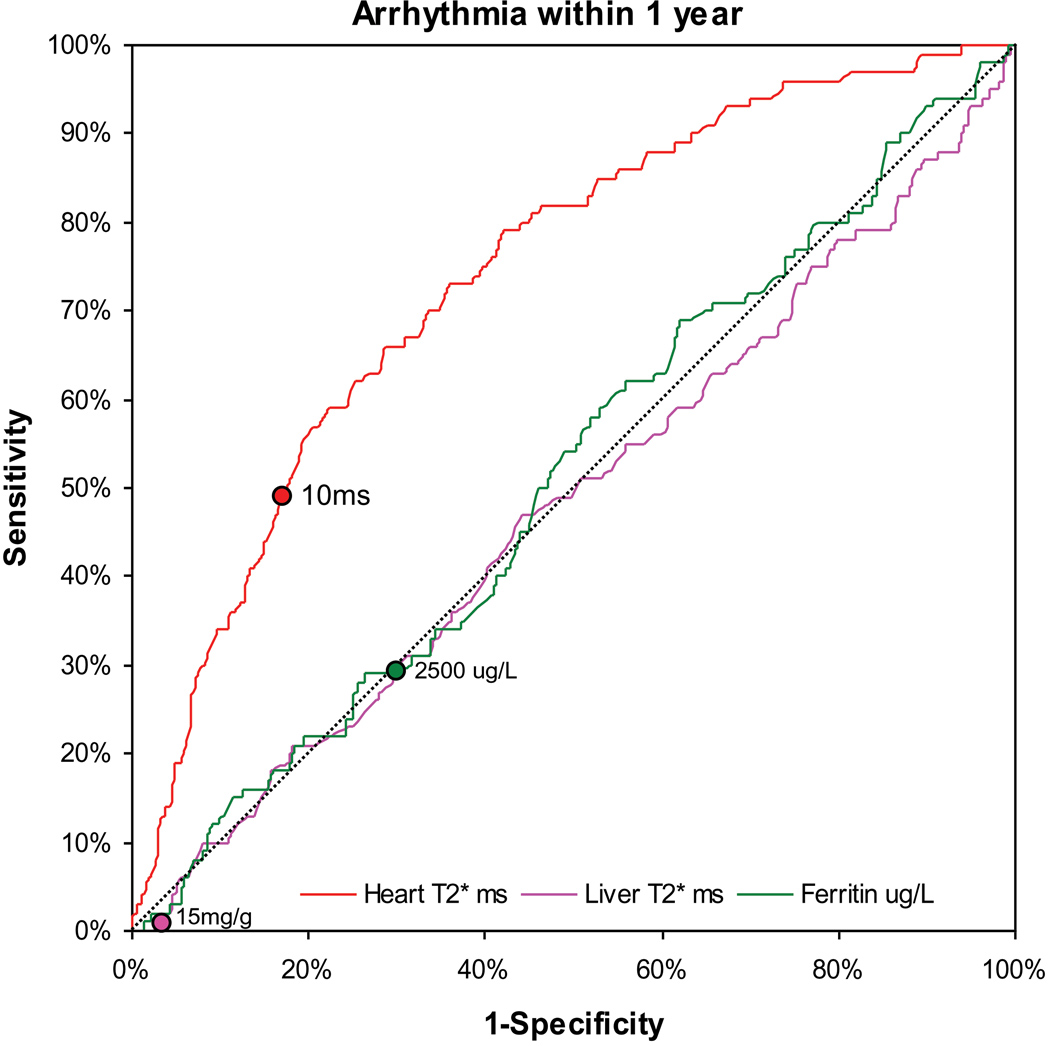
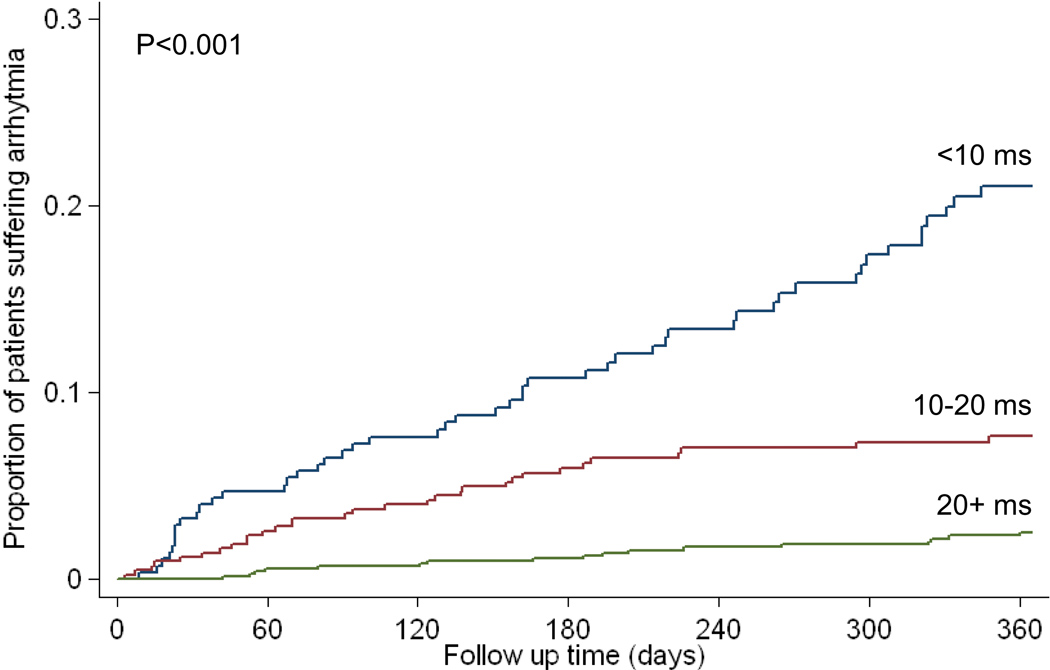
Methods and results: We analyzed cardiac and liver T2* magnetic resonance and serum ferritin in 652 thalassemia major patients from 21 UK centers with 1442 magnetic resonance scans. The relative risk for heart failure with cardiac T2* values <10 ms (compared with >10 ms) was 160 (95% confidence interval, 39 to 653). Heart failure occurred in 47% of patients within 1 year of a cardiac T2* <6 ms with a relative risk of 270 (95% confidence interval, 64 to 1129). The area under the receiver-operating characteristic curve for predicting heart failure was significantly greater for cardiac T2* (0.948) than for liver T2* (0.589; P<0.001) or serum ferritin (0.629; P<0.001). Cardiac T2* was <10 ms in 98% of scans in patients who developed heart failure. The relative risk for arrhythmia with cardiac T2* values <20 ms (compared with >20 ms) was 4.6 (95% confidence interval, 2.66 to 7.95). Arrhythmia occurred in 14% of patients within 1 year of a cardiac T2* of <6 ms. The area under the receiver-operating characteristic curve for predicting arrhythmia was significantly greater for cardiac T2* (0.747) than for liver T2* (0.514; P<0.001) or serum ferritin (0.518; P<0.001). The cardiac T2* was <20 ms in 83% of scans in patients who developed arrhythmia.
Conclusions: Cardiac T2* magnetic resonance identifies patients at high risk of heart failure and arrhythmia from myocardial siderosis in thalassemia major and is superior to serum ferritin and liver iron. Using cardiac T2* for the early identification and treatment of patients at risk is a logical means of reducing the high burden of cardiac mortality in myocardial siderosis. Clinical Trial Registration- URL: http://www.clinicaltrials.gov. Unique identifier: NCT00520559.
Conflict of interest statement
Figures
Comment in
-
History and current impact of cardiac magnetic resonance imaging on the management of iron overload.Circulation. 2009 Nov 17;120(20):1937-9. doi: 10.1161/CIRCULATIONAHA.109.907196. Epub 2009 Nov 2. Circulation. 2009. PMID: 19884464 Free PMC article. No abstract available.
References
-
- Weatherall DJ. Oxford Textbook of Medicine. Oxford University Press; 1996. Anaemia as a World Health Problem; pp. 3463–3482.
-
- Borgna-Pignatti C, Rugolotto S, De Stefano P, Zhao H, Cappellini MD, Del Vecchio GC, Romeo MA, Forni GL, Gamberini MR, Ghilardi R, Piga A, Cnaan A. Survival and complications in patients with thalassemia major treated with transfusion and deferoxamine. Haematologica. 2004;89:1187–1193. - PubMed
-
- Modell B, Khan M, Darlison M. Survival in beta thalassaemia major in the UK: data from the UK Thalassaemia Register. Lancet. 2000;355:2051–2052. - PubMed
-
- Olivieri NF, Nathan DG, MacMillan JH, Wayne AS, Liu PP, McGee A, Martin M, Koren G, Cohen AR. Survival in medically treated patients with homozygous beta-thalassemia. N Engl J Med. 1994;331:574–578. - PubMed
