

The same systemic autoimmune disease provokes arthritis and endocarditis via distinct mechanisms
- PMID: 19805369
- PMCID: PMC2757808
- DOI: 10.1073/pnas.0909132106
The same systemic autoimmune disease provokes arthritis and endocarditis via distinct mechanisms
Abstract
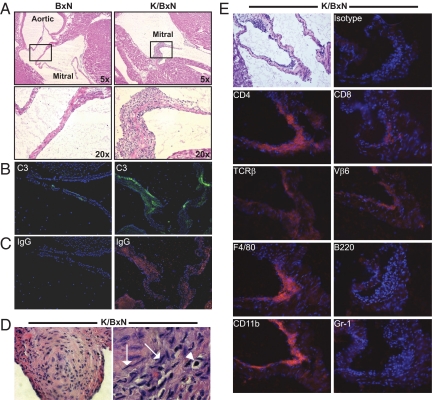
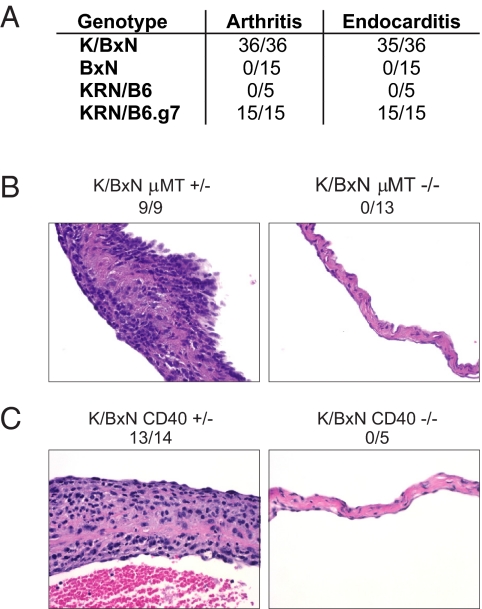
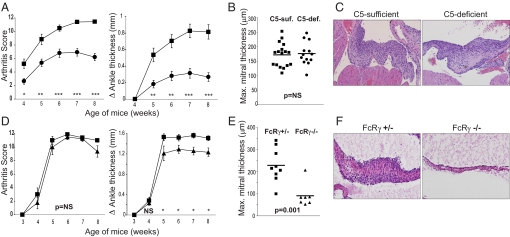
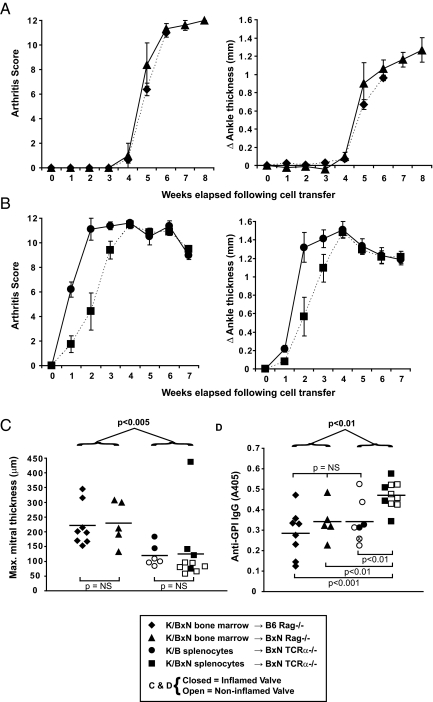
The immune mechanisms that provoke concomitant inflammation of synovial joints and cardiac valves in disorders such as rheumatic fever and systemic lupus erythematosus remain poorly defined. Here, we report the discovery of spontaneous endocarditis-in addition to their well-studied autoimmune arthritis-in K/BxN T cell receptor (TCR) transgenic mice. The same adaptive immune system elements were required for initiation of arthritis and endocarditis, and both diseases were dependent on autoantibodies. In contrast, the participation of key innate immune system molecules and perhaps T cells as effectors of inflammation differed between the 2 target tissues. Arthritis in K/BxN TCR transgenic mice depended primarily on complement C5 and not FcRgamma-using receptors; conversely, endocarditis depended essentially on FcRgamma receptors and not C5. Elucidating how a single systemic autoimmune disease engages distinct immune effector pathways to damage different target tissues is essential for optimizing the treatment of such disorders.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Autoantibody-mediated arthritis in the absence of C3 and activating Fcγ receptors: C5 is activated by the coagulation cascade.Arthritis Res Ther. 2012 Dec 13;14(6):R269. doi: 10.1186/ar4117. Arthritis Res Ther. 2012. PMID: 23237573 Free PMC article.
-
Fcγ receptor III and Fcγ receptor IV on macrophages drive autoimmune valvular carditis in mice.Arthritis Rheumatol. 2014 Apr;66(4):852-62. doi: 10.1002/art.38311. Arthritis Rheumatol. 2014. PMID: 24757138 Free PMC article.
-
Absence of β2 integrins impairs regulatory T cells and exacerbates CD4+ T cell-dependent autoimmune carditis.J Immunol. 2011 Sep 1;187(5):2702-10. doi: 10.4049/jimmunol.1000967. Epub 2011 Jul 27. J Immunol. 2011. PMID: 21795599 Free PMC article.
-
Initiation of an autoimmune response: insights from a transgenic model of rheumatoid arthritis.Immunol Res. 2005;32(1-3):5-13. doi: 10.1385/IR:32:1-3:005. Immunol Res. 2005. PMID: 16106055 Review.
-
The role and clinical implications of G6PI in experimental models of rheumatoid arthritis.Arthritis Res Ther. 2005;7(1):20-8. doi: 10.1186/ar1476. Epub 2004 Nov 30. Arthritis Res Ther. 2005. PMID: 15642150 Free PMC article. Review.
Cited by
-
Noninvasive ultrasound stimulation of the spleen to treat inflammatory arthritis.Nat Commun. 2019 Mar 12;10(1):951. doi: 10.1038/s41467-019-08721-0. Nat Commun. 2019. PMID: 30862842 Free PMC article.
-
Autoantibody-mediated arthritis in the absence of C3 and activating Fcγ receptors: C5 is activated by the coagulation cascade.Arthritis Res Ther. 2012 Dec 13;14(6):R269. doi: 10.1186/ar4117. Arthritis Res Ther. 2012. PMID: 23237573 Free PMC article.
-
Heart Inflammation: Immune Cell Roles and Roads to the Heart.Am J Pathol. 2019 Aug;189(8):1482-1494. doi: 10.1016/j.ajpath.2019.04.009. Epub 2019 May 18. Am J Pathol. 2019. PMID: 31108102 Free PMC article. Review.
-
Noninvasive Low-Frequency Pulsed Focused Ultrasound Therapy for Rheumatoid Arthritis in Mice.Research (Wash D C). 2022 Dec 19;2022:0013. doi: 10.34133/research.0013. eCollection 2022. Research (Wash D C). 2022. PMID: 39290964 Free PMC article.
-
Profibrotic VEGFR3-Dependent Lymphatic Vessel Growth in Autoimmune Valvular Carditis.Arterioscler Thromb Vasc Biol. 2024 Apr;44(4):807-821. doi: 10.1161/ATVBAHA.123.320326. Epub 2024 Jan 25. Arterioscler Thromb Vasc Biol. 2024. PMID: 38269589 Free PMC article.
References
-
- Chung CP, et al. Increased coronary-artery atherosclerosis in rheumatoid arthritis: Relationship to disease duration and cardiovascular risk factors. Arthritis Rheum. 2005;52:3045–3053. - PubMed
-
- Asanuma Y, et al. Premature coronary-artery atherosclerosis in systemic lupus erythematosus. N Engl J Med. 2003;349:2407–2415. - PubMed
-
- Blank M, Aron-Maor A, Shoenfeld Y. From rheumatic fever to Libman-Sacks endocarditis: Is there any possible pathogenetic link? Lupus. 2005;14:697–701. - PubMed
-
- Guilherme L, Kalil J, Cunningham M. Molecular mimicry in the autoimmune pathogenesis of rheumatic heart disease. Autoimmunity. 2006;39:31–39. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
