

Laparoscopy compared with laparotomy for comprehensive surgical staging of uterine cancer: Gynecologic Oncology Group Study LAP2
- PMID: 19805679
- PMCID: PMC2773219
- DOI: 10.1200/JCO.2009.22.3248
Laparoscopy compared with laparotomy for comprehensive surgical staging of uterine cancer: Gynecologic Oncology Group Study LAP2
Abstract
Purpose: The objective was to compare laparoscopy versus laparotomy for comprehensive surgical staging of uterine cancer.
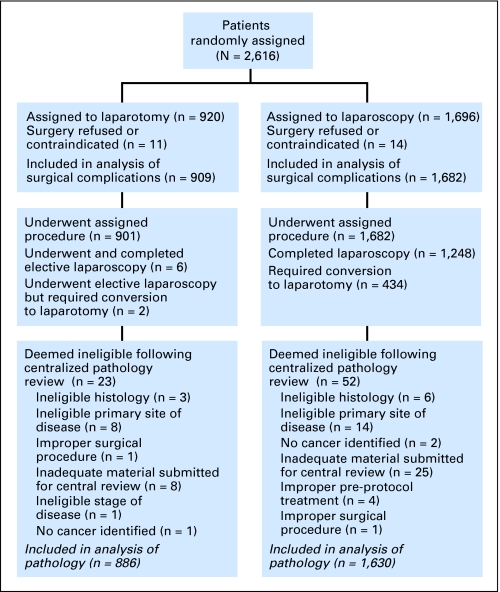
Patients and methods: Patients with clinical stage I to IIA uterine cancer were randomly assigned to laparoscopy (n = 1,696) or open laparotomy (n = 920), including hysterectomy, salpingo-oophorectomy, pelvic cytology, and pelvic and para-aortic lymphadenectomy. The main study end points were 6-week morbidity and mortality, hospital length of stay, conversion from laparoscopy to laparotomy, recurrence-free survival, site of recurrence, and patient-reported quality-of-life outcomes.
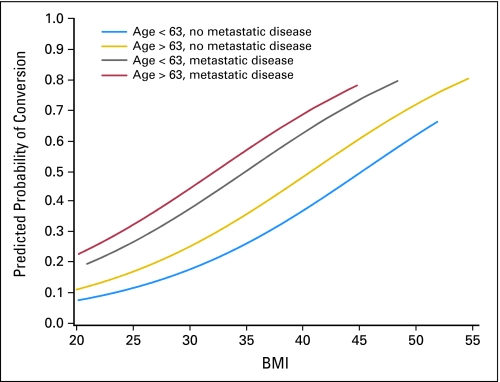
Results: Laparoscopy was initiated in 1,682 patients and completed without conversion in 1,248 patients (74.2%). Conversion from laparoscopy to laparotomy was secondary to poor visibility in 246 patients (14.6%), metastatic cancer in 69 patients (4.1%), bleeding in 49 patients (2.9%), and other cause in 70 patients (4.2%). Laparoscopy had fewer moderate to severe postoperative adverse events than laparotomy (14% v 21%, respectively; P < .0001) but similar rates of intraoperative complications, despite having a significantly longer operative time (median, 204 v 130 minutes, respectively; P < .001). Hospitalization of more than 2 days was significantly lower in laparoscopy versus laparotomy patients (52% v 94%, respectively; P < .0001). Pelvic and para-aortic nodes were not removed in 8% of laparoscopy patients and 4% of laparotomy patients (P < .0001). No difference in overall detection of advanced stage (stage IIIA, IIIC, or IVB) was seen (17% of laparoscopy patients v 17% of laparotomy patients; P = .841).
Conclusion: Laparoscopic surgical staging for uterine cancer is feasible and safe in terms of short-term outcomes and results in fewer complications and shorter hospital stay. Follow-up of these patients will determine whether surgical technique impacts pattern of recurrence or disease-free survival.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Is it safe to treat endometrial carcinoma endoscopically?J Clin Oncol. 2009 Nov 10;27(32):5305-7. doi: 10.1200/JCO.2009.23.9822. Epub 2009 Oct 5. J Clin Oncol. 2009. PMID: 19805666 No abstract available.
References
-
- American Cancer Society. Cancer facts and figures 2007. Atlanta, GA: American Cancer Society; 2007.
-
- Morrow CP, Bundy BN, Kurman FJ, et al. Relationship between surgical-pathological risk factors and outcome in clinical stage I and II carcinoma of the endometrium: A Gynecologic Oncology Group study. Gynecol Oncol. 1991;40:55–65. - PubMed
-
- Creasman WT, Morrow CP, Bundy BN, et al. Surgical pathologic spread patterns of endometrial cancer. Cancer. 1987;60:2035–2041. - PubMed
-
- Creasman WT, Odicino F, Maisonneuve P, et al. Carcinoma of the corpus uteri. Int J Gynaecol Obstet. 2003;83(suppl 1):79–118. - PubMed
-
- American Joint Committee on Cancer. Cancer Staging Manual. ed 6. New York, NY: Springer-Verlag; 2002.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
