

The video head impulse test: diagnostic accuracy in peripheral vestibulopathy
- PMID: 19805730
- PMCID: PMC2890997
- DOI: 10.1212/WNL.0b013e3181bacf85
The video head impulse test: diagnostic accuracy in peripheral vestibulopathy
Abstract
Background: The head impulse test (HIT) is a useful bedside test to identify peripheral vestibular deficits. However, such a deficit of the vestibulo-ocular reflex (VOR) may not be diagnosed because corrective saccades cannot always be detected by simple observation. The scleral search coil technique is the gold standard for HIT measurements, but it is not practical for routine testing or for acute patients, because they are required to wear an uncomfortable contact lens.
Objective: To develop an easy-to-use video HIT system (vHIT) as a clinical tool for identifying peripheral vestibular deficits. To validate the diagnostic accuracy of vHIT by simultaneous measures with video and search coil recordings across healthy subjects and patients with a wide range of previously identified peripheral vestibular deficits.
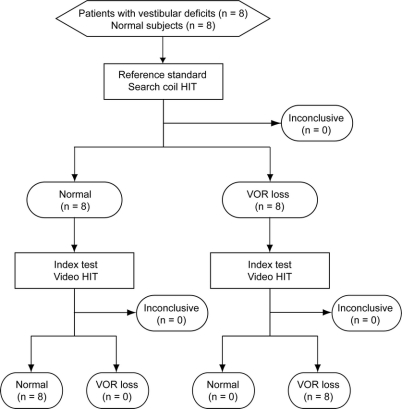
Methods: Horizontal HIT was recorded simultaneously with vHIT (250 Hz) and search coils (1,000 Hz) in 8 normal subjects, 6 patients with vestibular neuritis, 1 patient after unilateral intratympanic gentamicin, and 1 patient with bilateral gentamicin vestibulotoxicity.
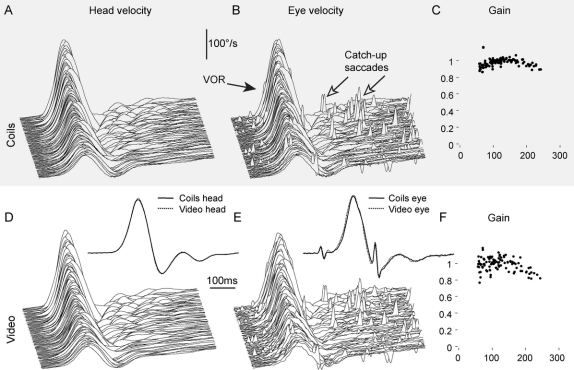
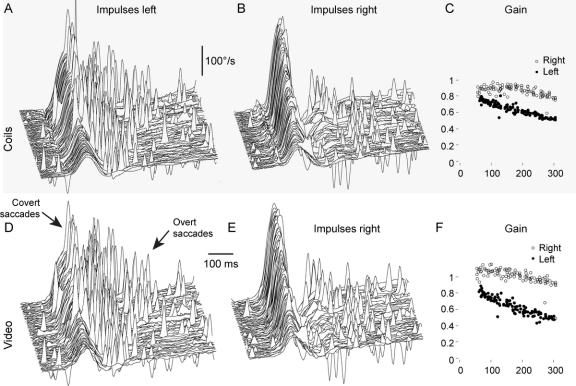
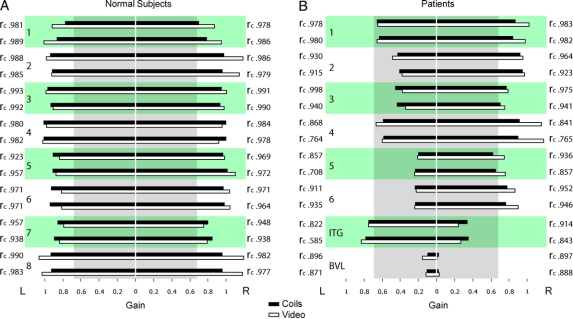
Results: Simultaneous video and search coil recordings of eye movements were closely comparable (average concordance correlation coefficient r(c) = 0.930). Mean VOR gains measured with search coils and video were not significantly different in normal (p = 0.107) and patients (p = 0.073). With these groups, the sensitivity and specificity of both the reference and index test were 1.0 (95% confidence interval 0.69-1.0). vHIT measures detected both overt and covert saccades as accurately as coils.
Conclusions: The video head impulse test is equivalent to search coils in identifying peripheral vestibular deficits but easier to use in clinics, even in patients with acute vestibular neuritis.
Figures
References
-
- Halmagyi GM, Curthoys IS. A clinical sign of canal paresis. Arch Neurol 1988;45:737–739. - PubMed
-
- Aw ST, Fetter M, Cremer PD, Karlberg M, Halmagyi GM. Individual semicircular canal function in superior and inferior vestibular neuritis. Neurology 2001;57:768–774. - PubMed
-
- Black RA, Halmagyi GM, Thurtell MJ, Todd MJ, Curthoys IS. The active head-impulse test in unilateral peripheral vestibulopathy. Arch Neurol 2005;62:290–293. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical