

Is maximum conservative management an equivalent treatment option to dialysis for elderly patients with significant comorbid disease?
- PMID: 19808244
- PMCID: PMC2758251
- DOI: 10.2215/CJN.00510109
Is maximum conservative management an equivalent treatment option to dialysis for elderly patients with significant comorbid disease?
Abstract
Background and objectives: There is ongoing growth of elderly populations with ESRD in Western Europe and North America. In our center, we offer an alternative care pathway of 'maximum conservative management' (MCM) to patients who elect not to start dialysis, often because of a heavy burden of comorbid illness and advanced age. The objective of our study was to compare clinical outcomes for patients who had ESRD and chose either MCM or renal replacement therapy (RRT).
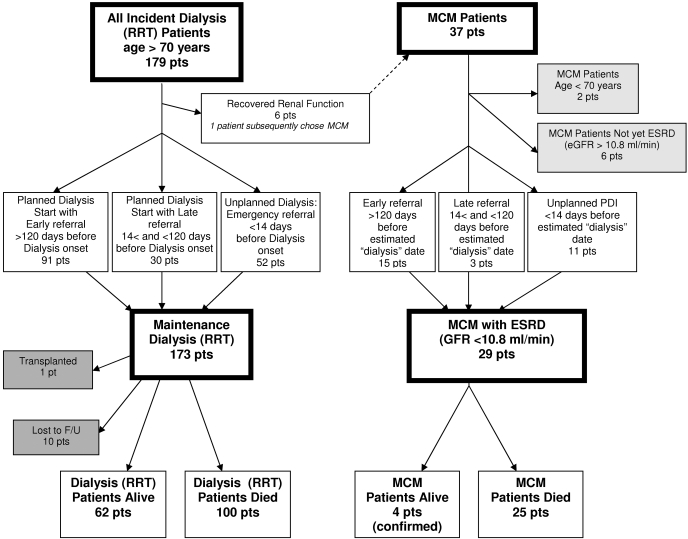
Design, setting, participants, & measurements: This is an observational study of a single-center cohort in the United Kingdom that evaluating 202 elderly (> or =70 yr) patients who had ESRD and had chosen either MCM (n = 29) or RRT (n = 173). We report survival, hospitalization rates, and location of death for this cohort. Survival was measured from a standardized 'threshold' estimated GFR of 10.8 ml/min per 1.73 m(2).
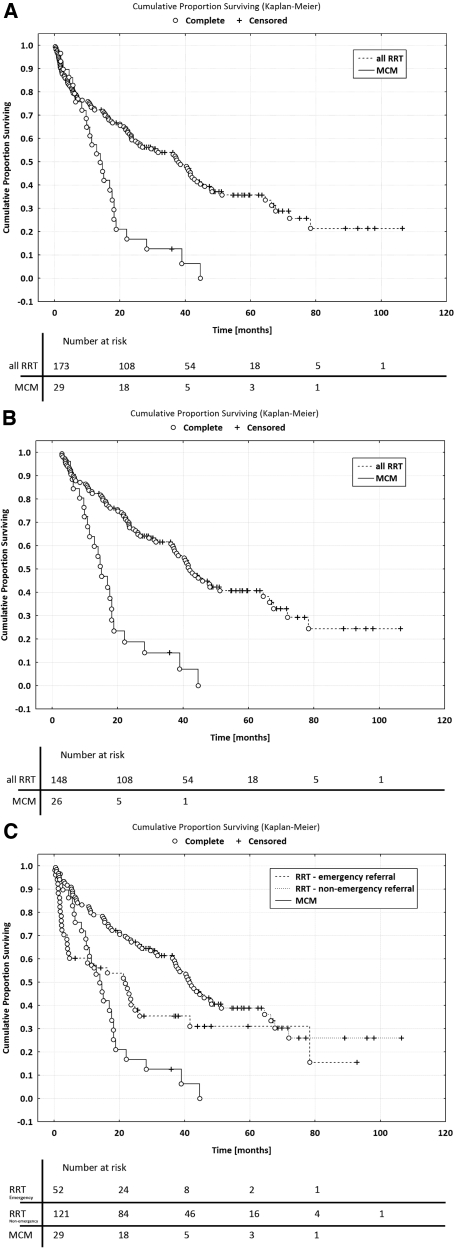
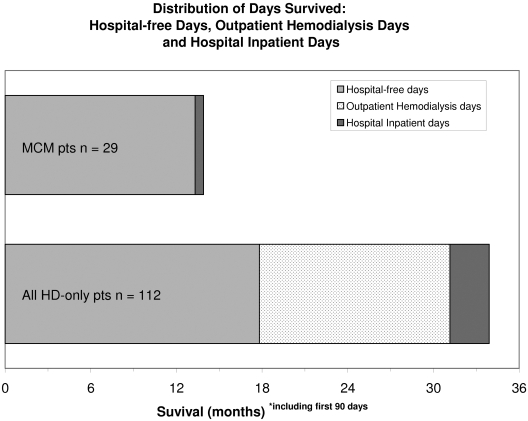
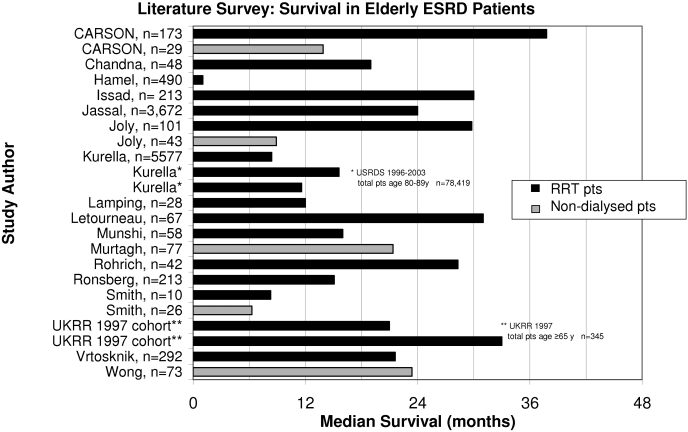
Results: Median survival, including the first 90 d, was 37.8 mo (range 0 to 106 mo) for RRT patients and 13.9 mo (range 2 to 44) for MCM patients (P < 0.01). RRT patients had higher rates of hospitalization (0.069 [95% confidence interval (CI) 0.068 to 0.070]) versus 0.043 [95% CI 0.040 to 0.047] hospital days/patient-days survived) compared with MCM patients. MCM patients were significantly more likely to die at home or in a hospice (odds ratio 4.15; 95% CI 1.67 to 10.25). A survey of the literature describing elderly ESRD outcomes is also presented.
Conclusions: Dialysis prolongs survival for elderly patients who have ESRD with significant comorbidity by approximately 2 yr; however, patients who choose MCM can survive a substantial length of time, achieving similar numbers of hospital-free days to patients who choose hemodialysis.
Figures
References
-
- Farrington K, Rao R, Gilg J, Ansell D, Feest T: Chapter 3: New adult patients starting renal replacement therapy in the UK in 2005. In: UK Renal Registry: The Ninth Annual Report, edited by Ansell D, Feest T, Hodsman A, Rao R, Tomson C, Udayaraj U, Williams A, Warwick G.Bristol, United Kingdom, The Renal Association, 2006, pp 15– 41
-
- Kurella M, Covinsky KE, Collins AJ, Chertow GM: Octogenarians and nonagenarians starting dialysis in the United States. Ann Intern Med 146: 177– 183, 2007 - PubMed
-
- Collins AJ, Foley R, Herzog C, Chavers B, Gilbertson D, Ishani A, Kasiske B, Liu J, Mau LW, Mcbean M, Murray A, St. Peter W, Xue J, Fan Q, Guo H, Li Q, Li S, Peng Y, Qiu Y, Roberts T, Skeans M, Snyder J, Solid C, Wang C, Weinhandl E, Zaun D, Zhang R, Arko C, Chen SC, Dalleska F, Daniels F, Dunning S, Ebben J, Frazier E, Hanzlik C, Johnson R, Sheets D, Wang X, Forrest B, Constantini E, Everson S, Eggers P, Agodoa L: Excerpts from the United States Renal Data System 2007 annual data report: ESRD incidence and prevalence. Am J Kidney Dis 51: S81– S98, 2008 - PubMed
-
- Collins AJ, Foley R, Herzog C, Chavers B, Gilbertson D, Ishani A, Kasiske B, Liu J, Mau LW, Mcbean M, Murray A, St. Peter W, Xue J, Fan Q, Guo H, Li Q, Li S, Peng Y, Qiu Y, Roberts T, Skeans M, Snyder J, Solid C, Wang C, Weinhandl E, Zaun D, Zhang R, Arko C, Chen SC, Dalleska F, Daniels F, Dunning S, Ebben J, Frazier E, Hanzlik C, Johnson R, Sheets D, Wang X, Forrest B, Constantini E, Everson S, Eggers P, Agodoa L: Excerpts from the United States Renal Data System 2007 annual data report: Emerging issues. Am J Kidney Dis 51: S33– S48, 2008 - PubMed
-
- Krishnan M, Lok CE, Jassal SV: Epidemiology and demographic aspects of treated end-stage renal disease in the elderly. Semin Dial 15: 79– 83, 2002 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
