

Metabolic syndrome, inflammation, and incident heart failure in the elderly: the cardiovascular health study
- PMID: 19808298
- PMCID: PMC2762642
- DOI: 10.1161/CIRCHEARTFAILURE.108.785485
Metabolic syndrome, inflammation, and incident heart failure in the elderly: the cardiovascular health study
Abstract
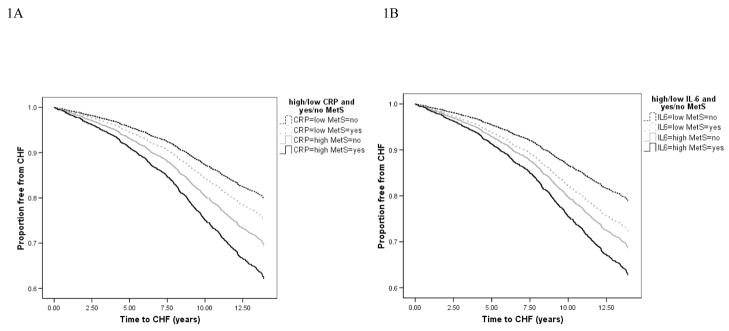
Background: Inflammation markers and metabolic syndrome (MetS) are associated with risk of congestive heart failure (CHF). We evaluated whether combining inflammation markers and MetS provided additive information for incident CHF and if incorporating inflammation markers to the MetS definition added prognostic information.
Methods and results: We studied 4017 men and women > or =65 years old, without baseline CHF or diabetes, participating in the Cardiovascular Health Study, an observational study with 12.2 years follow-up and 966 cases of incident CHF. Baseline "C-reactive protein (CRP)-MetS" or "interleukin (IL)-6-MetS" were defined as presence of 3 out of 6 components, with elevated CRP (> or =3 mg/L) or IL-6 (> or =2.21 pg/mL) as a sixth component added to ATPIII criteria. Cox models adjusted for CHF risk factors and incident coronary disease were used to calculate hazard ratios for CHF. MetS and elevated inflammation markers were independently associated with CHF risk (hazard ratios, 95% CI: 1.32, 1.16 to 1.51 for MetS; 1.53, 1.34 to 1.75 for CRP; 1.37, 1.19 to 1.55 for IL-6). There was a 20% relative excess risk attributed to the combination of MetS and CRP (95% CI, -44% to 88%). CRP-MetS and IL-6-MetS definitions reclassified 18% and 13%, respectively of participants as MetS. Both CRP-MetS and IL-6-MetS increased risk of CHF by 60% compared with those without MetS.
Conclusions: MetS and inflammation markers provided additive information on CHF risk in this elderly cohort. Inflammation-incorporated MetS definitions identified more participants with the same risk level as ATPIII MetS. Considering inflammation markers and MetS together may be useful in clinical and research settings.
Figures
References
-
- Thom T, Haase N, Rosamond W, Howard VJ, Rumsfeld J, Manolio T, Zheng ZJ, Flegal K, O'Donnell C, Kittner S, Lloyd-Jones D, Goff DC, Jr, Hong Y, Adams R, Friday G, Furie K, Gorelick P, Kissela B, Marler J, Meigs J, Roger V, Sidney S, Sorlie P, Steinberger J, Wasserthiel-Smoller S, Wilson M, Wolf P. Heart disease and stroke statistics--2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2006;113(6):e85–151. - PubMed
-
- Ho KK, Pinsky JL, Kannel WB, Levy D. The epidemiology of heart failure: the Framingham Study. J Am Coll Cardiol. 1993;22(4 Suppl A):6A–13A. - PubMed
-
- Ingelsson E, Sundstrom J, Arnlov J, Zethelius B, Lind L. Insulin resistance and risk of congestive heart failure. JAMA. 2005;294(3):334–41. - PubMed
-
- Barzilay JI, Kronmal RA, Gottdiener JS, Smith NL, Burke GL, Tracy R, Savage PJ, Carlson M. The association of fasting glucose levels with congestive heart failure in diabetic adults > or =65 years: the Cardiovascular Health Study. J Am Coll Cardiol. 2004;43(12):2236–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01-HC-85085/HC/NHLBI NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- N01-HC-85081/HC/NHLBI NIH HHS/United States
- N01-HC-85086/HC/NHLBI NIH HHS/United States
- N01-HC-85082/HC/NHLBI NIH HHS/United States
- N01 HC-55222/HC/NHLBI NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- N01-HC-85079/HC/NHLBI NIH HHS/United States
- N01 HC075150/HL/NHLBI NIH HHS/United States
- N01 HC045133/HC/NHLBI NIH HHS/United States
- N01 HC035129/HC/NHLBI NIH HHS/United States
- N01-HC-85084/HC/NHLBI NIH HHS/United States
- N01 HC015103/HC/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- N01-HC-85083/HC/NHLBI NIH HHS/United States
- N01-HC-75150/HC/NHLBI NIH HHS/United States
- N01-HC-85080/HC/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
