

Prognostic value of biomarkers in heart failure: application of novel methods in the community
- PMID: 19808368
- PMCID: PMC2774116
- DOI: 10.1161/CIRCHEARTFAILURE.109.849299
Prognostic value of biomarkers in heart failure: application of novel methods in the community
Abstract
Background: Mortality among patients with heart failure is high. Though individual biomarkers have been investigated to determine their value in mortality risk prediction, the role of a multimarker strategy requires further evaluation.
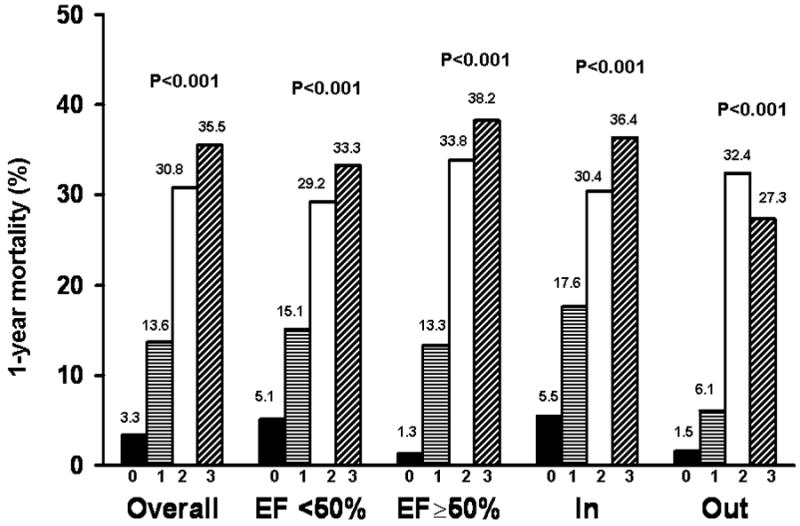
Methods and results: Olmsted County residents presenting with heart failure from July 2004 to September 2007 were recruited to undergo biomarker measurement. We investigated whether addition of C-reactive protein, B-type natriuretic peptide, and troponin T to a model including established risk indicators improved 1-year mortality risk prediction using the c statistic, integrated discrimination improvement, and net reclassification improvement. Among 593 participants, the mean age was 76.4 years, and 48% were men. After 1 year of follow-up, 122 (20.6%) participants had died. Patients with C-reactive protein (<11.8 mg/L), B-type natriuretic peptide (<350 pg/mL), and troponin T (< or = 0.01 ng/mL) less than the median had low 1-year mortality (3.3%), whereas those with 2 or 3 biomarkers greater than the median had markedly increased mortality (30.8% and 35.5%, respectively). The addition of 2 or more biomarkers to the model offered greater improvement in 1-year mortality risk prediction than use of a single biomarker. The combination of C-reactive protein and B-type natriuretic peptide resulted in an increase in the c statistic from 0.757 to 0.810 (P<0.001), an integrated discrimination improvement gain of 7.1% (P<0.001), and a net reclassification improvement of 22.1% (P<0.001). Use of all 3 biomarkers offered no incremental gain (integrated discrimination improvement gain 0.7% versus C-reactive protein+B-type natriuretic peptide, P=0.065).
Conclusions: Biomarkers improved 1-year mortality risk prediction beyond established indicators. The use of a 2-biomarker combination was superior to a single biomarker in risk prediction, though addition of a third biomarker conferred no added benefit.
Figures
Comment in
-
Are multiple biomarker testing strategies ready for prime time in heart failure?Circ Heart Fail. 2009 Sep;2(5):387-8. doi: 10.1161/CIRCHEARTFAILURE.109.898429. Circ Heart Fail. 2009. PMID: 19808366 No abstract available.
References
-
- Association AH, editor. Heart Disease and Stroke Statistics 2008 Update. 2008.
-
- Roger VL, Weston SA, Redfield MM, Hellermann-Homan JP, Killian J, Yawn BP, Jacobsen SJ. Trends in heart failure incidence and survival in a community-based population. Jama. 2004;292:344–50. - PubMed
-
- Levy D, Kenchaiah S, Larson MG, Benjamin EJ, Kupka MJ, Ho KK, Murabito JM, Vasan RS. Long-term trends in the incidence of and survival with heart failure. N Engl J Med. 2002;347:1397–402. - PubMed
-
- Fonarow GC. Epidemiology and risk stratification in acute heart failure. Am Heart J. 2008;155:200–7. - PubMed
-
- Mueller C, Laule-Kilian K, Christ A, Brunner-La Rocca HP, Perruchoud AP. Inflammation and long-term mortality in acute congestive heart failure. Am Heart J. 2006;151:845–50. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
