

Age-related left ventricular remodeling and associated risk for cardiovascular outcomes: the Multi-Ethnic Study of Atherosclerosis
- PMID: 19808592
- PMCID: PMC2744970
- DOI: 10.1161/CIRCIMAGING.108.819938
Age-related left ventricular remodeling and associated risk for cardiovascular outcomes: the Multi-Ethnic Study of Atherosclerosis
Abstract
Background: Age-related alterations of left ventricular (LV) structure and function that may predispose to cardiovascular events are not well understood.
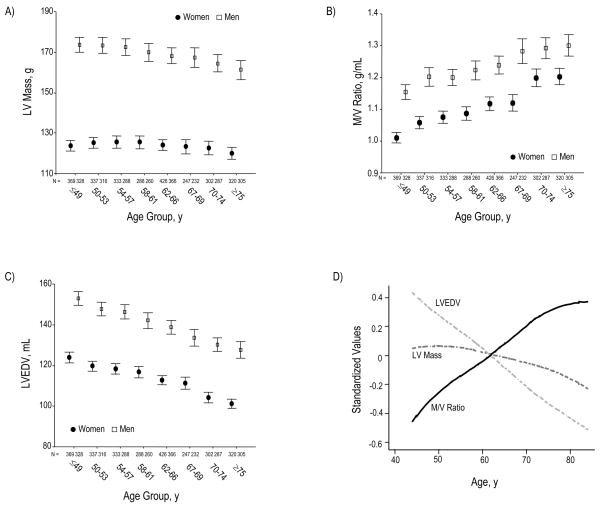
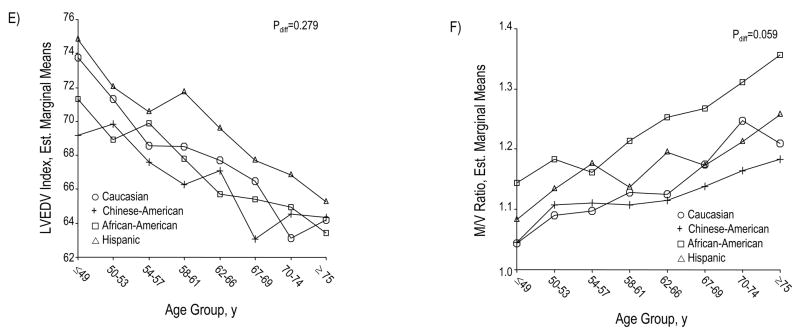
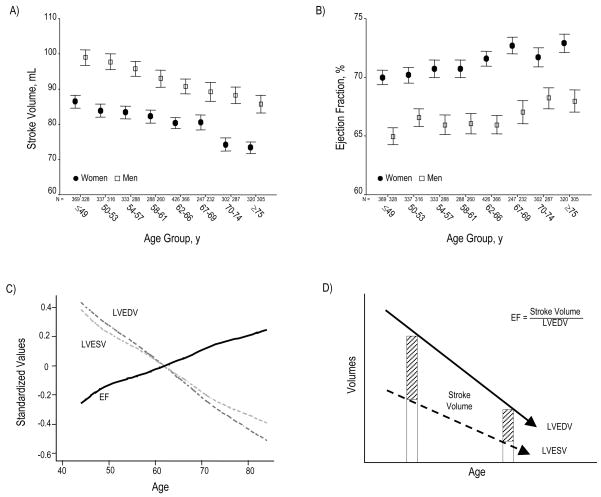
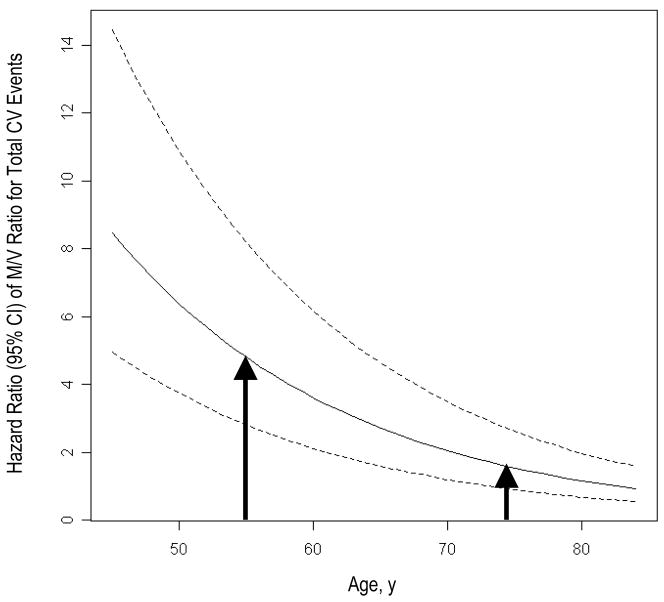
Methods and results: We used cardiac MRI to examine age-related differences in LV structure and function in 5004 participants without overt cardiovascular disease when enrolled in the Multi-Ethnic Study of Atherosclerosis; 1099 participants received additional strain analyses by MRI tagging. We also assessed the relation of age-associated remodeling with cardiovascular outcomes using Cox proportional hazard models adjusting for cardiovascular risk factors. Although LV mass decreased with age (-0.3 g per year), the mass-to-volume ratio markedly increased (+5 mg/mL per year, P<0.0001), driven by a substantial reduction in end-diastolic volume (-0.8 mL per year, P<0.0001). Age was also associated with a significant fall in stroke volume (-0.4 mL per year, P<0.0001), along with strain patterns reflecting systolic (P<0.0001) as well as diastolic (P<0.01) myocardial dysfunction-despite a modestly enhanced ejection fraction (+0.1% per year, P<0.0001). Increased mass-to-volume ratio conferred a significant risk for total cardiovascular events; this trend was strongest among younger (<65 years; hazard ratio, 3.69 [CI, 1.34 to 10.10]) versus older (> or =65 years; hazard ratio, 1.68 [CI 0.77 to 3.68]) individuals with the highest compared to lowest mass-to-volume ratio quintile (P(interaction)=0.013).
Conclusions: Age is associated with a phenotype of LV remodeling marked by increased mass-to-volume ratio and accompanied by systolic as well as diastolic myocardial dysfunction that is not reflected by preserved ejection fraction. This pattern of ventricular remodeling confers significant cardiovascular risk, particularly when present earlier in life.
Figures
References
-
- Lakatta EG, Levy D. Arterial and cardiac aging: major shareholders in cardiovascular disease enterprises: Part I: aging arteries: a “set up” for vascular disease. Circulation. 2003;107:139–46. - PubMed
-
- Lakatta EG, Levy D. Arterial and cardiac aging: major shareholders in cardiovascular disease enterprises: Part II: the aging heart in health: links to heart disease. Circulation. 2003;107:346–54. - PubMed
-
- Lakatta EG. Arterial and cardiac aging: major shareholders in cardiovascular disease enterprises: Part III: cellular and molecular clues to heart and arterial aging. Circulation. 2003;107:490–7. - PubMed
-
- Dannenberg AL, Levy D, Garrison RJ. Impact of age on echocardiographic left ventricular mass in a healthy population (the Framingham Study) Am J Cardiol. 1989;64:1066–8. - PubMed
-
- Lindroos M, Kupari M, Heikkila J, Tilvis R. Echocardiographic evidence of left ventricular hypertrophy in a general aged population. Am J Cardiol. 1994;74:385–90. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
